Theodor Eugen Oprea, Carmen Gabriela Barbu, Sorina Carmen Martin, Anca Elena Sarbu, Simona Gabriela Duta, Irina Manuela Nistor, Simona Fica
{"title":"Degraded Bone Microarchitecture in Women with PHPT-Significant Predictor of Fracture Probability.","authors":"Theodor Eugen Oprea, Carmen Gabriela Barbu, Sorina Carmen Martin, Anca Elena Sarbu, Simona Gabriela Duta, Irina Manuela Nistor, Simona Fica","doi":"10.1177/11795514221145840","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Patients with primary hyperparathyroidism (PHPT) experience bone mineral density (BMD) loss and trabecular bone score (TBS) alteration, which current guidelines recommend assessing. Considering TBS alongside BMD for a 10-year fracture risk assessment (FRAX) may improve PHPT management.</p><p><strong>Design: </strong>Retrospective, cross-sectional study composed of 49 Caucasian females (62 ± 10.6 years, 27.7 ± 0.87 kg/m<sup>2</sup>) with PHPT and 132 matched control subjects (61.3 ± 10.5 years, 27.5 ± 0.49 kg/m<sup>2</sup>) evaluated in 3 years. We assessed lumbar spine (LS) and femoral neck (FN) BMD, T and Z scores (GE Healthcare Lunar Osteodensitometer) and TBS (iNsight 1.8), major osteoporotic fracture (MOF), and hip FRAX.</p><p><strong>Results: </strong>Patients with PHPT had statistically lower mean values for lumbar spine bone mineral density (LS BMD) (0.95 ± 0.25 vs 1.01 ± 0.14 g/cm<sup>2</sup>, <i>P</i> = .01), LS T-scores (-2 ± 0.2 vs -1.4 ± 0.1 SD, <i>P</i> = .009), LS Z scores (-0.9 ± 0.19 vs -0.1 ± 0.11 SD, <i>P</i> = .009), femoral neck bone mineral density (FN BMD) (0.79 ± 0.02 vs 0.83 ± 0.01 g/cm<sup>2</sup>, <i>P</i> = .02), FN T-scores (-1.8 ± 0.13 vs -1.5 ± 0.07 SD, <i>P</i> = .017), FN Z scores (-0.51 ± 0.87 vs -0.1 ± 0.82 SD, <i>P</i> = .006), and TBS (0.95 ± 0.25 vs 1.01 ± 0.14 g/cm<sup>2</sup>, <i>P</i> = .01) compared with control subjects. 22.4% of patients with PHPT had degraded microarchitecture (TBS < 1.2) vs. 7.6% in control group (χ<sup>2</sup> = 0.008). PHPT proved to be a covariate with unique contribution (<i>P</i> = .031) alongside LS BMD (<i>P</i> = .040) in a linear regression model [<i>R</i> <sup>2</sup> = 0.532, <i>F(4,16)</i> = 4.543] for TBS < 1.2. TBS adjustment elevated MOF FRAX both for PHPT (4.35 ± 0.6% vs 5.25% ± 0.73%, <i>P</i> < .001) and control groups (4.5 ± 0.24% vs 4.7% ± 0.26%, <i>P</i> < .001) compared with BMD-bases FRAX, but also increased differently between the 2 study groups (1.1-folds for PHPT patients and 1.04 for control subjects, <i>P</i> = .034).</p><p><strong>Conclusion: </strong>Compared with control, TBS-adjusted FRAX provides significantly higher MOF risk than BMD-based FRAX in PHPT women.</p>","PeriodicalId":44715,"journal":{"name":"Clinical Medicine Insights-Endocrinology and Diabetes","volume":"16 ","pages":"11795514221145840"},"PeriodicalIF":3.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/79/10/10.1177_11795514221145840.PMC9869236.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Endocrinology and Diabetes","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795514221145840","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Patients with primary hyperparathyroidism (PHPT) experience bone mineral density (BMD) loss and trabecular bone score (TBS) alteration, which current guidelines recommend assessing. Considering TBS alongside BMD for a 10-year fracture risk assessment (FRAX) may improve PHPT management.
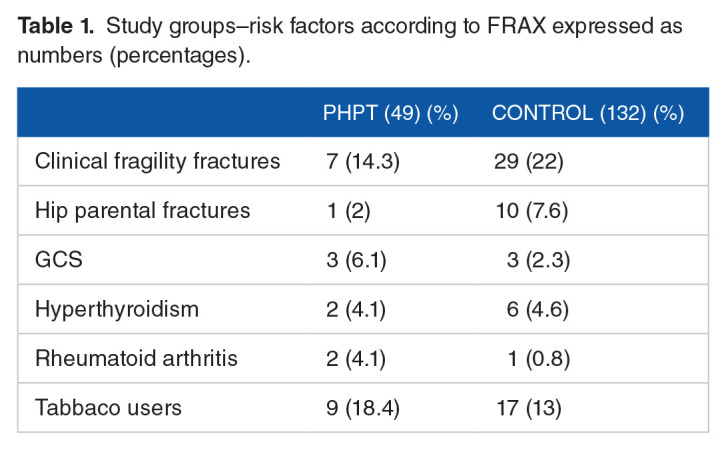
Design: Retrospective, cross-sectional study composed of 49 Caucasian females (62 ± 10.6 years, 27.7 ± 0.87 kg/m2) with PHPT and 132 matched control subjects (61.3 ± 10.5 years, 27.5 ± 0.49 kg/m2) evaluated in 3 years. We assessed lumbar spine (LS) and femoral neck (FN) BMD, T and Z scores (GE Healthcare Lunar Osteodensitometer) and TBS (iNsight 1.8), major osteoporotic fracture (MOF), and hip FRAX.
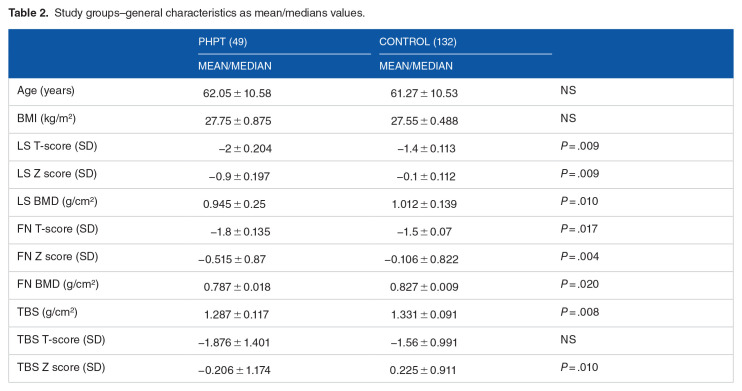
Results: Patients with PHPT had statistically lower mean values for lumbar spine bone mineral density (LS BMD) (0.95 ± 0.25 vs 1.01 ± 0.14 g/cm2, P = .01), LS T-scores (-2 ± 0.2 vs -1.4 ± 0.1 SD, P = .009), LS Z scores (-0.9 ± 0.19 vs -0.1 ± 0.11 SD, P = .009), femoral neck bone mineral density (FN BMD) (0.79 ± 0.02 vs 0.83 ± 0.01 g/cm2, P = .02), FN T-scores (-1.8 ± 0.13 vs -1.5 ± 0.07 SD, P = .017), FN Z scores (-0.51 ± 0.87 vs -0.1 ± 0.82 SD, P = .006), and TBS (0.95 ± 0.25 vs 1.01 ± 0.14 g/cm2, P = .01) compared with control subjects. 22.4% of patients with PHPT had degraded microarchitecture (TBS < 1.2) vs. 7.6% in control group (χ2 = 0.008). PHPT proved to be a covariate with unique contribution (P = .031) alongside LS BMD (P = .040) in a linear regression model [R2 = 0.532, F(4,16) = 4.543] for TBS < 1.2. TBS adjustment elevated MOF FRAX both for PHPT (4.35 ± 0.6% vs 5.25% ± 0.73%, P < .001) and control groups (4.5 ± 0.24% vs 4.7% ± 0.26%, P < .001) compared with BMD-bases FRAX, but also increased differently between the 2 study groups (1.1-folds for PHPT patients and 1.04 for control subjects, P = .034).
Conclusion: Compared with control, TBS-adjusted FRAX provides significantly higher MOF risk than BMD-based FRAX in PHPT women.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


