{"title":"Glioma diagnosis and comprehensive management during COVID-19 pandemic: A proposed algorithm.","authors":"Cindy Cecilia, Djohan Ardiansyah","doi":"10.25259/JNRP_45_2022","DOIUrl":null,"url":null,"abstract":"<p><p>The coronavirus disease 2019 (COVID-19) has significantly changed the health-care system. COVID-19 patients with comorbidities are more likely to have severe disease, often leading to death. As one primary concern in this pandemic era, glioma patients have an incidence of 30%. It has a high mortality rate. Glioma has multiple comorbidities, at risk of contracting COVID-19, such as elderly, taking high-dose steroid therapy with adjuvant radiotherapy (RT) and chemotherapy. An algorithm for patient-doctor communication, inpatient-outpatient selection, and treatment goals in glioma patients should be carefully made according to local preparation for COVID-19. Surgery, RT, and chemotherapy should be tailored individually to increase survival rate, quality of life, and reduce the risk of COVID-19 exposure. All communication between the health-care provider and patient will be using telemedicine. The patient who requires to visit the inpatient ward will be carefully selected. Asymptomatic glioma or with no progressivity of the disease should have the treatment postponed. Symptomatic high-grade glioma patients with progressive neurological deficits and increased intracranial pressure will be treated with COVID-19 protocols. Surgery, RT, and chemotherapy, especially Temozolomide, will be given after evaluating the patient's age, Karnofsky Performance Scale (KPS) Score, and molecular finding of O6-methylguanine DNA methyltransferase (MGMT), isocitrate dehydrogenase, and gene 1p/9q. Therefore, it is necessary to have a modified algorithm for glioma patients during this pandemic.</p><p><strong>Key messages: </strong>A strategy to minimize hospital contact for glioma patients in a pandemic crisis while not delaying their diagnostics and treatments.</p>","PeriodicalId":16443,"journal":{"name":"Journal of Neurosciences in Rural Practice","volume":"14 3","pages":"395-398"},"PeriodicalIF":0.8000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10483201/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurosciences in Rural Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/JNRP_45_2022","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/16 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
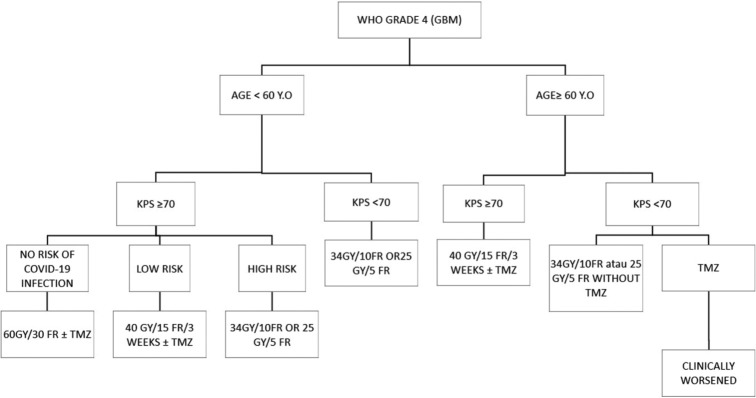
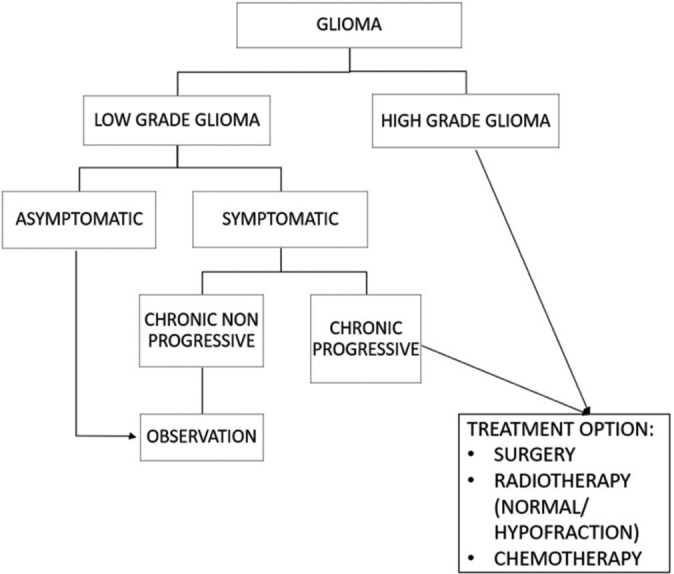
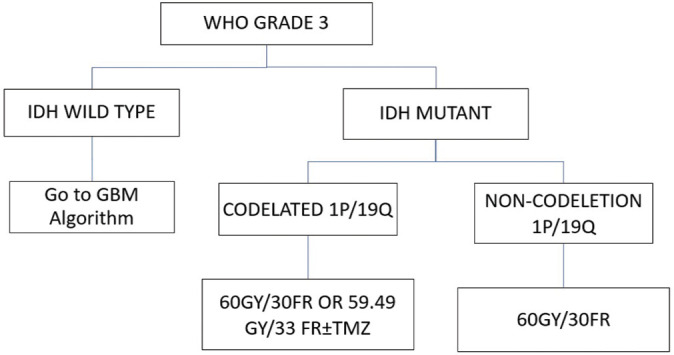
The coronavirus disease 2019 (COVID-19) has significantly changed the health-care system. COVID-19 patients with comorbidities are more likely to have severe disease, often leading to death. As one primary concern in this pandemic era, glioma patients have an incidence of 30%. It has a high mortality rate. Glioma has multiple comorbidities, at risk of contracting COVID-19, such as elderly, taking high-dose steroid therapy with adjuvant radiotherapy (RT) and chemotherapy. An algorithm for patient-doctor communication, inpatient-outpatient selection, and treatment goals in glioma patients should be carefully made according to local preparation for COVID-19. Surgery, RT, and chemotherapy should be tailored individually to increase survival rate, quality of life, and reduce the risk of COVID-19 exposure. All communication between the health-care provider and patient will be using telemedicine. The patient who requires to visit the inpatient ward will be carefully selected. Asymptomatic glioma or with no progressivity of the disease should have the treatment postponed. Symptomatic high-grade glioma patients with progressive neurological deficits and increased intracranial pressure will be treated with COVID-19 protocols. Surgery, RT, and chemotherapy, especially Temozolomide, will be given after evaluating the patient's age, Karnofsky Performance Scale (KPS) Score, and molecular finding of O6-methylguanine DNA methyltransferase (MGMT), isocitrate dehydrogenase, and gene 1p/9q. Therefore, it is necessary to have a modified algorithm for glioma patients during this pandemic.
Key messages: A strategy to minimize hospital contact for glioma patients in a pandemic crisis while not delaying their diagnostics and treatments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


