Samuel Schick, Alex Dombrowsky, Jamal Egbaria, Kyle D Paul, Eugene Brabston, Amit Momaya, Brent Ponce
{"title":"Variability in physical therapy protocols following total shoulder arthroplasty.","authors":"Samuel Schick, Alex Dombrowsky, Jamal Egbaria, Kyle D Paul, Eugene Brabston, Amit Momaya, Brent Ponce","doi":"10.5397/cise.2023.00115","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Physical therapy (PT) plays an important role in the recovery of function following anatomic total shoulder arthroplasty (aTSA). While several PT protocols have been published for these patients, there is no standardized protocol for aTSA rehabilitation. This lack of standardization may lead to confusion between patients and physicians, possibly resulting in suboptimal outcomes. This study examines how PT protocols provided by academic orthopedic surgery programs vary regarding therapeutic goals and activities following aTSA.</p><p><strong>Methods: </strong>PT protocols for aTSA available online from the Accreditation Council for Graduate Medical Education accredited orthopedic surgery programs were included for review. Each protocol was analyzed to evaluate it for differences in recommendation of length of immobilization, range of motion (ROM) goals, start time for and progression of therapeutic exercises, and timing for return to functional activity.</p><p><strong>Results: </strong>Of 175 accredited programs, 25 (14.2%) had protocols publicly available, programs (92%) recommended sling immobilization outside of therapy for an average of 4.4±2.0 weeks. Most protocols gave recommendations on starting active forward flexion (24 protocols, range 1-7 weeks), external rotation (22 protocols, range 1-7 weeks), and internal rotation (18 protocols, range 4-7 weeks). Full passive ROM was recommended at 10.8±5.7 weeks, and active ROM was 13.3±3.9 weeks, on average. ROM goals were inconsistent among protocols, with significant variations in recommended ROM and resistance exercise start times. Only 13 protocols (52%) gave recommendations on resuming recreational activities (mean, 17.4±4.4 weeks).</p><p><strong>Conclusions: </strong>Publicly available PT protocols for aTSA rehabilitation are highly variable. Level of evidence: IV.</p>","PeriodicalId":33981,"journal":{"name":"Clinics in Shoulder and Elbow","volume":"26 3","pages":"267-275"},"PeriodicalIF":1.8000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8a/9a/cise-2023-00115.PMC10497930.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics in Shoulder and Elbow","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5397/cise.2023.00115","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Physical therapy (PT) plays an important role in the recovery of function following anatomic total shoulder arthroplasty (aTSA). While several PT protocols have been published for these patients, there is no standardized protocol for aTSA rehabilitation. This lack of standardization may lead to confusion between patients and physicians, possibly resulting in suboptimal outcomes. This study examines how PT protocols provided by academic orthopedic surgery programs vary regarding therapeutic goals and activities following aTSA.
Methods: PT protocols for aTSA available online from the Accreditation Council for Graduate Medical Education accredited orthopedic surgery programs were included for review. Each protocol was analyzed to evaluate it for differences in recommendation of length of immobilization, range of motion (ROM) goals, start time for and progression of therapeutic exercises, and timing for return to functional activity.
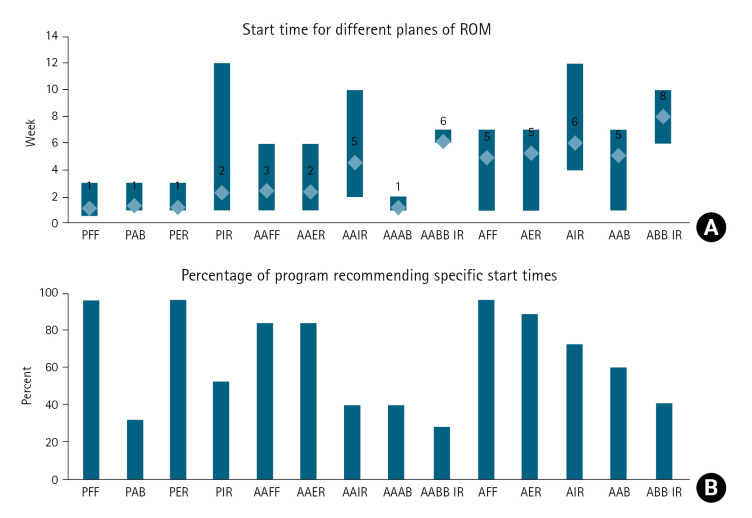
Results: Of 175 accredited programs, 25 (14.2%) had protocols publicly available, programs (92%) recommended sling immobilization outside of therapy for an average of 4.4±2.0 weeks. Most protocols gave recommendations on starting active forward flexion (24 protocols, range 1-7 weeks), external rotation (22 protocols, range 1-7 weeks), and internal rotation (18 protocols, range 4-7 weeks). Full passive ROM was recommended at 10.8±5.7 weeks, and active ROM was 13.3±3.9 weeks, on average. ROM goals were inconsistent among protocols, with significant variations in recommended ROM and resistance exercise start times. Only 13 protocols (52%) gave recommendations on resuming recreational activities (mean, 17.4±4.4 weeks).
Conclusions: Publicly available PT protocols for aTSA rehabilitation are highly variable. Level of evidence: IV.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


