{"title":"A systematic review of the efficacy of ketamine for craniofacial pain.","authors":"Yasmine Hoydonckx, Tyler McKechnie, Miki Peer, Marina Englesakis, Pranab Kumar","doi":"10.1080/24740527.2023.2210167","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Craniofacial pain (CFP) poses a burden on patients and health care systems. It is hypothesized that ketamine, an <i>N</i>-methyl-d-aspartate (NMDA) receptor antagonist, can reverse central sensitization associated with causation and propagation of CFP. This systematic review aims to assess the role of ketamine for CFP.</p><p><strong>Methods: </strong>Databases were searched for studies published up to September 26, 2022, investigating the efficacy of ketamine for adults with CFP. Primary outcome was the change in pain intensity at 60 min postintervention. Two reviewers screened and extracted data. Registration with PROSPERO was performed (CRD42020178649).</p><p><strong>Results: </strong>Twenty papers (six randomized controlled trials [RCTs], 14 observational studies) including 670 patients were identified. Substantial heterogeneity in terms of study design, population, dose, route of administration, treatment duration, and follow-up was noted. Bolus dose ranged from 0.2-0.3 mg/kg (intravenous) to 0.4 mg/kg (intramuscular) to 0.25-0.75 mg/kg (intranasal). Ketamine infusions (0.1-1 mg/kg/h) were given over various durations. Follow-up was short in RCTs (from 60 min to 72 h) but longer in observational studies (up to 18 months). Ketamine by bolus treatment failed to reduce migraine intensity but had an effect by reducing intensity of aura, cluster headache (CH), and trigeminal neuralgia. Prolonged ketamine infusions showed sustainable reduction of migraine intensity and frequency of CH attacks, but the quality of the evidence is low.</p><p><strong>Conclusion: </strong>Current evidence remains conflicting on the efficacy of ketamine for CFP owing to low quality and heterogeneity across studies. Ketamine infusions are suggested to provide sustained improvement, possibly because of prolonged duration and higher dosage of administration. RCTs should focus on the dose-response relationship of prolonged ketamine infusions on CFP.</p>","PeriodicalId":53214,"journal":{"name":"Canadian Journal of Pain-Revue Canadienne de la Douleur","volume":"7 1","pages":"2210167"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10294769/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Pain-Revue Canadienne de la Douleur","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/24740527.2023.2210167","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Craniofacial pain (CFP) poses a burden on patients and health care systems. It is hypothesized that ketamine, an N-methyl-d-aspartate (NMDA) receptor antagonist, can reverse central sensitization associated with causation and propagation of CFP. This systematic review aims to assess the role of ketamine for CFP.
Methods: Databases were searched for studies published up to September 26, 2022, investigating the efficacy of ketamine for adults with CFP. Primary outcome was the change in pain intensity at 60 min postintervention. Two reviewers screened and extracted data. Registration with PROSPERO was performed (CRD42020178649).
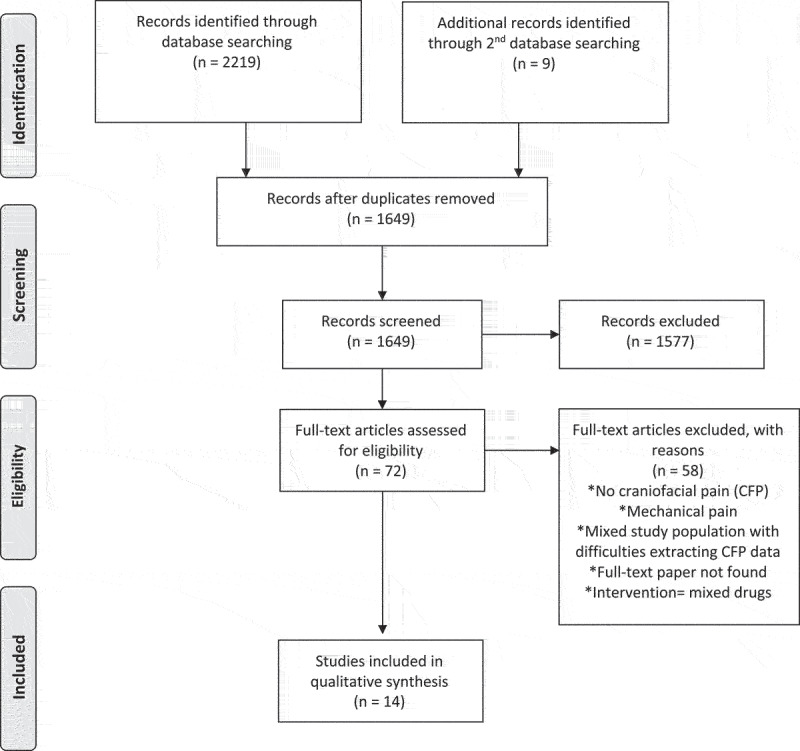
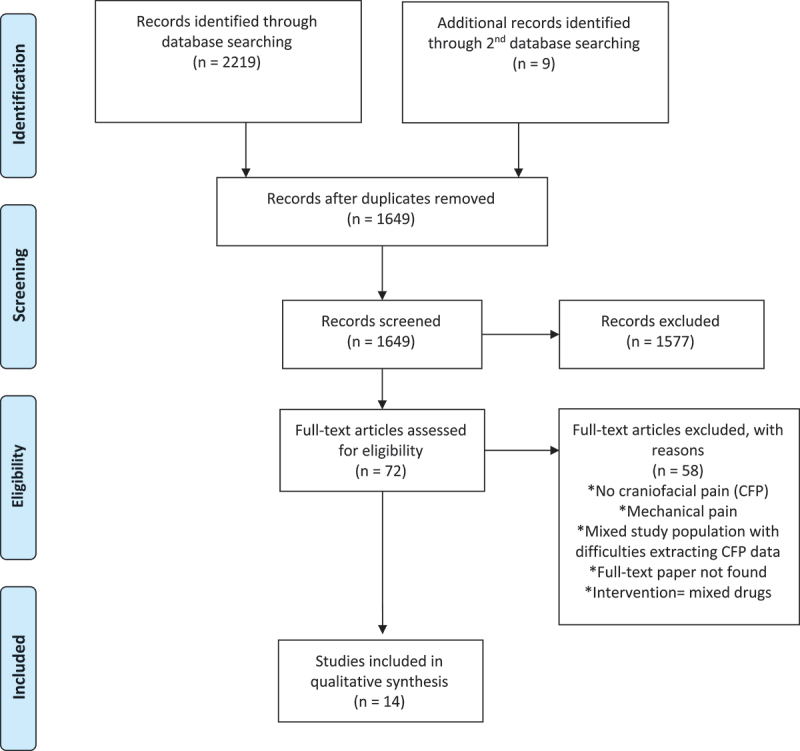
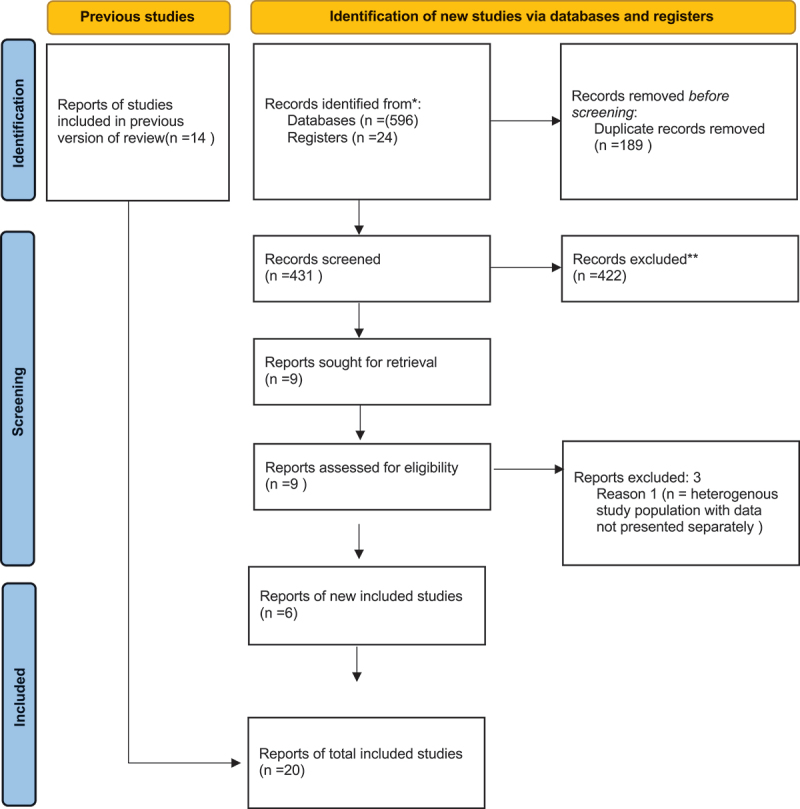
Results: Twenty papers (six randomized controlled trials [RCTs], 14 observational studies) including 670 patients were identified. Substantial heterogeneity in terms of study design, population, dose, route of administration, treatment duration, and follow-up was noted. Bolus dose ranged from 0.2-0.3 mg/kg (intravenous) to 0.4 mg/kg (intramuscular) to 0.25-0.75 mg/kg (intranasal). Ketamine infusions (0.1-1 mg/kg/h) were given over various durations. Follow-up was short in RCTs (from 60 min to 72 h) but longer in observational studies (up to 18 months). Ketamine by bolus treatment failed to reduce migraine intensity but had an effect by reducing intensity of aura, cluster headache (CH), and trigeminal neuralgia. Prolonged ketamine infusions showed sustainable reduction of migraine intensity and frequency of CH attacks, but the quality of the evidence is low.
Conclusion: Current evidence remains conflicting on the efficacy of ketamine for CFP owing to low quality and heterogeneity across studies. Ketamine infusions are suggested to provide sustained improvement, possibly because of prolonged duration and higher dosage of administration. RCTs should focus on the dose-response relationship of prolonged ketamine infusions on CFP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


