Fractures around the shoulder in the skeletally immature: A scoping review.
IF 2
Q2 ORTHOPEDICS
引用次数: 0
Abstract
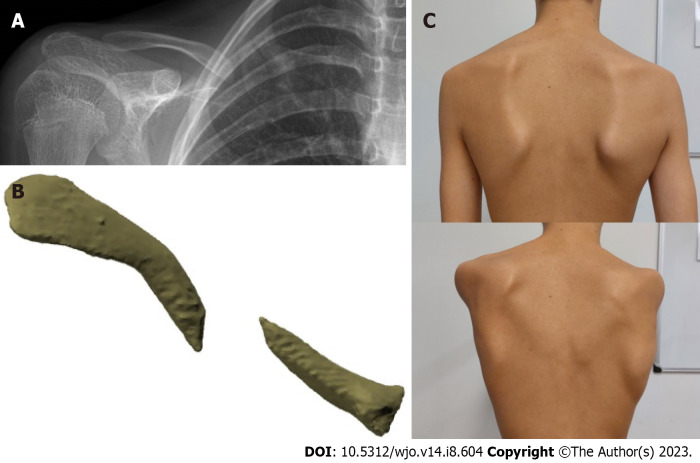
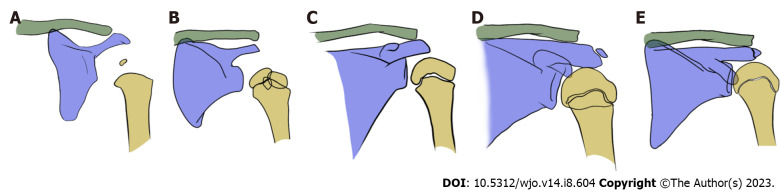
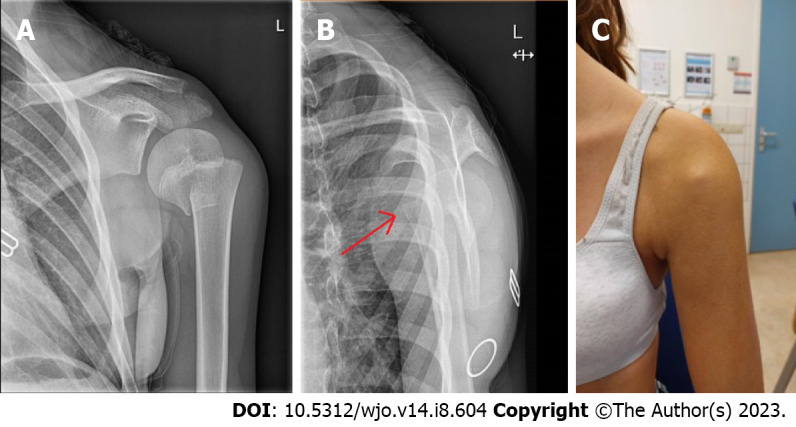
Fractures around the shoulder girdle in children are mainly caused by sports accidents. The clavicle and the proximal humerus are most commonly involved. Both the clavicle and the proximal humerus have a remarkable potential for remodeling, which is why most of these fractures in children can be treated conservatively. However, the key is to understand when a child benefits from surgical management. Clear indications for surgery of these fractures are lacking. This review focuses on the available evidence on the management of clavicle and proximal humerus fractures in children. The only strict indications for surgery for diaphyseal clavicle fractures in children are open fractures, tenting of the skin with necrosis, associated neurovascular injury, or a floating shoulder. There is no evidence to argue for surgery of displaced clavicle fractures to prevent malunion since most malunions are asymptomatic. In the rare case of a symptomatic malunion of the clavicle in children, corrective osteosynthesis is a viable treatment option. For proximal humerus fractures in children, treatment is dictated by the patient's age (and thus remodeling potential) and the amount of fracture displacement. Under ten years of age, even severely displaced fractures can be treated conservatively. From the age of 13 and onwards, surgery has better outcomes for severely displaced (Neer types III and IV) fractures. Between 10 and 13 years of age, the indications for surgical treatment are less clear, with varying cut-off values of angulation (30-60 degrees) or displacement (1/3 – 2/3 shaft width) in the current literature.
骨未成熟患者肩周骨折:范围回顾。
儿童肩带周围骨折主要是由运动事故引起的。锁骨和肱骨近端最常受累。锁骨和肱骨近端都有显著的重建潜力,这就是为什么大多数儿童骨折可以保守治疗的原因。然而,关键是要了解孩子什么时候能从手术治疗中受益。这些骨折缺乏明确的手术适应症。这篇综述的重点是关于儿童锁骨和肱骨近端骨折治疗的现有证据。儿童锁骨骨干骨折手术的唯一严格指征是开放性骨折、伴有坏死的皮肤支帐篷、相关的神经血管损伤或浮肩。没有证据表明移位的锁骨骨折手术可以预防畸形愈合,因为大多数畸形愈合是无症状的。在罕见的情况下,有症状的儿童锁骨畸形愈合,矫正骨整合是一个可行的治疗选择。对于儿童肱骨近端骨折,治疗取决于患者的年龄(以及重塑潜力)和骨折移位的程度。在10岁以下,即使是严重移位的骨折也可以保守治疗。从13岁起,手术治疗严重移位(III型和IV型除外)骨折的效果更好。在10 - 13岁之间,手术治疗的适应症不太明确,目前文献中有不同的截角值(30-60度)或位移(1/3 - 2/3轴宽)。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


