Michael Rothkopf, Mohan Pant, Rebecca Brown, Jaimie Haselhorst, Francine Gagliardotto, Allison Tallman, Debbie Stevenson, Andrew DePalma, Michael Saracco, Dan Rosenberg, Vladimir Proudan, Kishwar Shareef, Nudrat Ayub
{"title":"Impact of a multidisciplinary nutritional support team on quality improvement for patients receiving home parenteral nutrition.","authors":"Michael Rothkopf, Mohan Pant, Rebecca Brown, Jaimie Haselhorst, Francine Gagliardotto, Allison Tallman, Debbie Stevenson, Andrew DePalma, Michael Saracco, Dan Rosenberg, Vladimir Proudan, Kishwar Shareef, Nudrat Ayub","doi":"10.1136/bmjnph-2022-000484","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Home parenteral nutrition (HPN) is essential for patients with intestinal failure requiring long-term nutritional support. The Amerita Quality Improvement Project for HPN Patients (QIP-PN) explored the effect of a physician nutrition expert (PNE)-led multidisciplinary nutritional support team (MNST) on HPN care for patients under its service.</p><p><strong>Objective: </strong>To determine an MNST effect on adherence to protocols, outcomes and quality of life (QOL) in HPN.</p><p><strong>Methods: </strong>The study was divided into three phases: data review (phases 1a and 1b), observation (phase 2) and intervention (phase 3). Seven Amerita locations were selected as 'study branches' (population), from which all study patients and controls were drawn. The quality improvement project employed a quasi-experimental case-matched control group (control) design. Data were collected on demographics, treating physicians PNE status, HPN care variables, recommended interventions, quality-of-life assessment, adverse outcomes and hospitalisations. Paired t-test compared continuous data between phases 2 and 3. Comparisons between study and control groups used a negative binomial regression model.</p><p><strong>Results: </strong>Thirty-four patients were reviewed in phase 1a and 197 in phase 1b. Forty study patients completed phase 2 and progressed into phase 3, of whom 30 completed ≥60 therapy days. Patients were lost to follow-up if they discontinued HPN for any reason. Improvements in weight, body mass index and QOL were seen in the study patients during intervention. Recommendations made and accepted by treating physicians differed based on PNE status. Study patients had fewer adverse outcomes and related hospitalisations than controls.</p><p><strong>Conclusion: </strong>MNST recommendations improved clinical, biochemical parameters and patients' self-reported overall health. MNST input reduced adverse outcomes, hospitalisation and the length of stay at the hospital. This study highlights the potential for MNST to have a significant impact on the quality and overall cost of HPN management.</p>","PeriodicalId":36307,"journal":{"name":"BMJ Nutrition, Prevention and Health","volume":null,"pages":null},"PeriodicalIF":3.3000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/94/01/bmjnph-2022-000484.PMC9813622.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Nutrition, Prevention and Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjnph-2022-000484","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"NUTRITION & DIETETICS","Score":null,"Total":0}
引用次数: 1
Abstract
Introduction: Home parenteral nutrition (HPN) is essential for patients with intestinal failure requiring long-term nutritional support. The Amerita Quality Improvement Project for HPN Patients (QIP-PN) explored the effect of a physician nutrition expert (PNE)-led multidisciplinary nutritional support team (MNST) on HPN care for patients under its service.
Objective: To determine an MNST effect on adherence to protocols, outcomes and quality of life (QOL) in HPN.
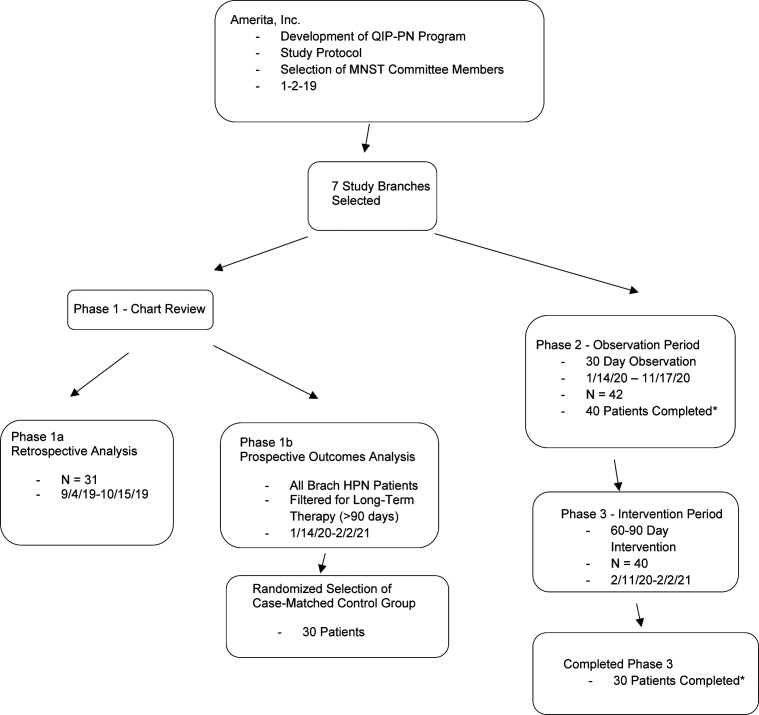
Methods: The study was divided into three phases: data review (phases 1a and 1b), observation (phase 2) and intervention (phase 3). Seven Amerita locations were selected as 'study branches' (population), from which all study patients and controls were drawn. The quality improvement project employed a quasi-experimental case-matched control group (control) design. Data were collected on demographics, treating physicians PNE status, HPN care variables, recommended interventions, quality-of-life assessment, adverse outcomes and hospitalisations. Paired t-test compared continuous data between phases 2 and 3. Comparisons between study and control groups used a negative binomial regression model.
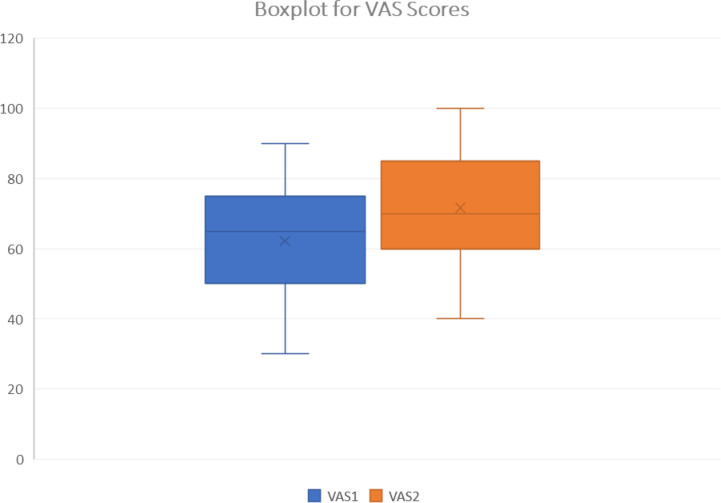
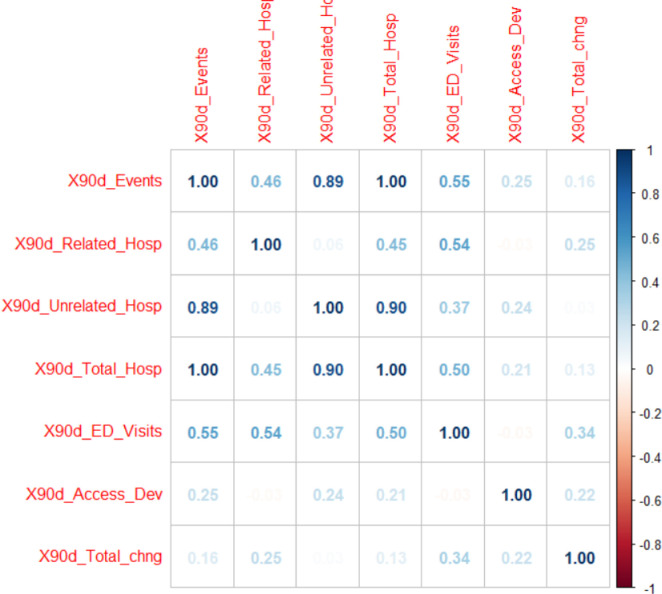
Results: Thirty-four patients were reviewed in phase 1a and 197 in phase 1b. Forty study patients completed phase 2 and progressed into phase 3, of whom 30 completed ≥60 therapy days. Patients were lost to follow-up if they discontinued HPN for any reason. Improvements in weight, body mass index and QOL were seen in the study patients during intervention. Recommendations made and accepted by treating physicians differed based on PNE status. Study patients had fewer adverse outcomes and related hospitalisations than controls.
Conclusion: MNST recommendations improved clinical, biochemical parameters and patients' self-reported overall health. MNST input reduced adverse outcomes, hospitalisation and the length of stay at the hospital. This study highlights the potential for MNST to have a significant impact on the quality and overall cost of HPN management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


