Adding low dose cyclophosphamide to rituximab for remission-induction may prolong relapse-free survival in patients with ANCA vasculitis: A retrospective study
Renée Ysermans , Matthias H. Busch , Joop P. Aendekerk , Jan G.M.C. Damoiseaux , Pieter van Paassen
{"title":"Adding low dose cyclophosphamide to rituximab for remission-induction may prolong relapse-free survival in patients with ANCA vasculitis: A retrospective study","authors":"Renée Ysermans , Matthias H. Busch , Joop P. Aendekerk , Jan G.M.C. Damoiseaux , Pieter van Paassen","doi":"10.1016/j.jtauto.2022.100178","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>Rituximab (RTX) and cyclophosphamide (CYC) are effective remission-induction therapies in anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV). However, combining these therapies may favor prognosis in patients with a major disease presentation. We conducted a retrospective study to compare patients treated with a combination of RTX and low dose CYC (RTX-CYC) or with RTX only, both followed by tailored maintenance with RTX, with regard to long-term outcomes.</p></div><div><h3>Methods</h3><p>Patients treated in the Maastricht University Medical Center between March 2007 and January 2019, were screened for eligibility. The primary outcome variable was major relapse rate after two and five years. Secondary outcome variables were clinical data and laboratory parameters.</p></div><div><h3>Results</h3><p>Of the 246 screened patients, 34 received RTX-CYC and 28 RTX only for remission-induction. All patients were followed for at least two years, with a median follow-up of 48 months (IQR 24–60). At baseline, renal involvement was more prevalent in the RTX-CYC patients (85% vs. 61%, <em>P</em> = 0.028). Major relapse rates within two years, but not after five years, were significantly lower in the RTX-CYC group (3% vs. 24%, <em>P</em> = 0.032). The rate of infections, hypogammaglobulinemia, end-stage renal disease, malignancies, and mortality did not differ after two and five years.</p></div><div><h3>Conclusion</h3><p>Adding low dose CYC to RTX is safe and may prevent major relapses in patients with severe AAV in the first two years after remission-induction. Randomized controlled trials that compare the efficacy and safety between RTX and a combination of RTX with CYC are needed.</p></div>","PeriodicalId":36425,"journal":{"name":"Journal of Translational Autoimmunity","volume":"6 ","pages":"Article 100178"},"PeriodicalIF":4.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9800337/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Translational Autoimmunity","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2589909022000399","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
Rituximab (RTX) and cyclophosphamide (CYC) are effective remission-induction therapies in anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV). However, combining these therapies may favor prognosis in patients with a major disease presentation. We conducted a retrospective study to compare patients treated with a combination of RTX and low dose CYC (RTX-CYC) or with RTX only, both followed by tailored maintenance with RTX, with regard to long-term outcomes.
Methods
Patients treated in the Maastricht University Medical Center between March 2007 and January 2019, were screened for eligibility. The primary outcome variable was major relapse rate after two and five years. Secondary outcome variables were clinical data and laboratory parameters.
Results
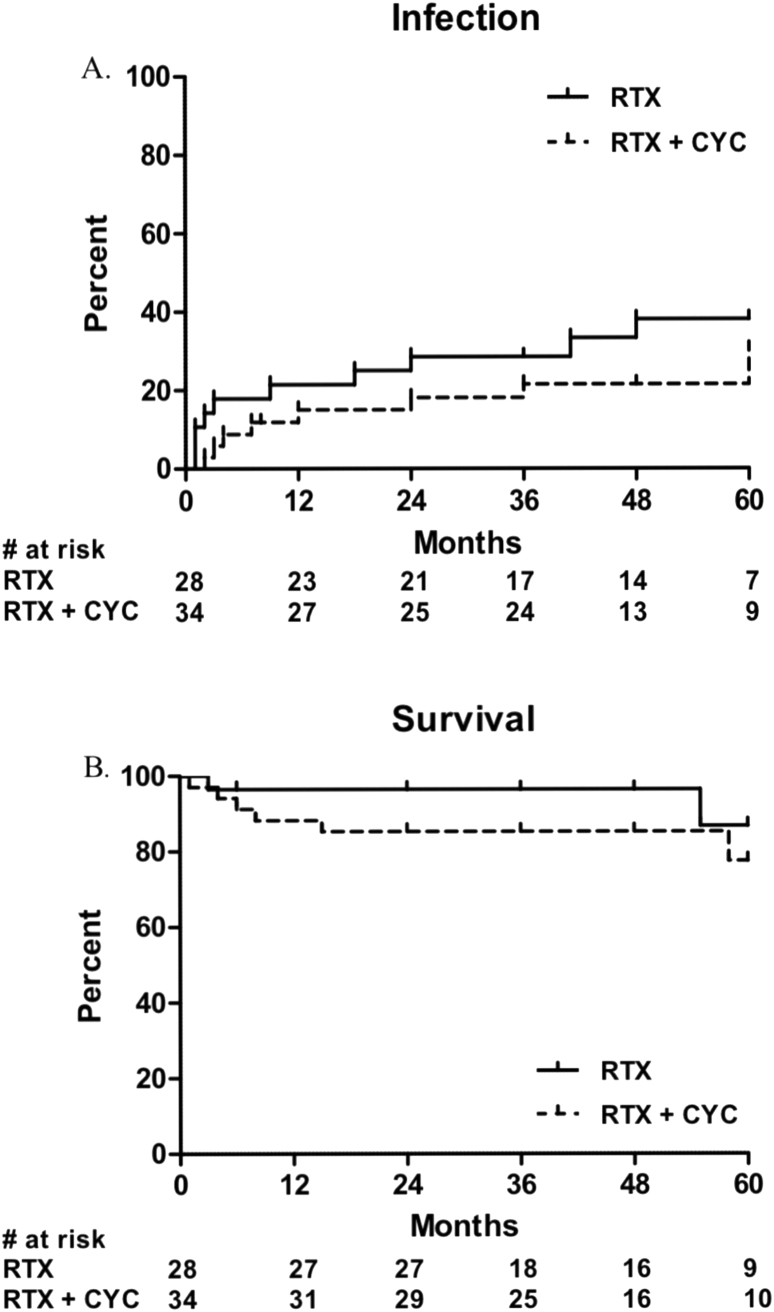
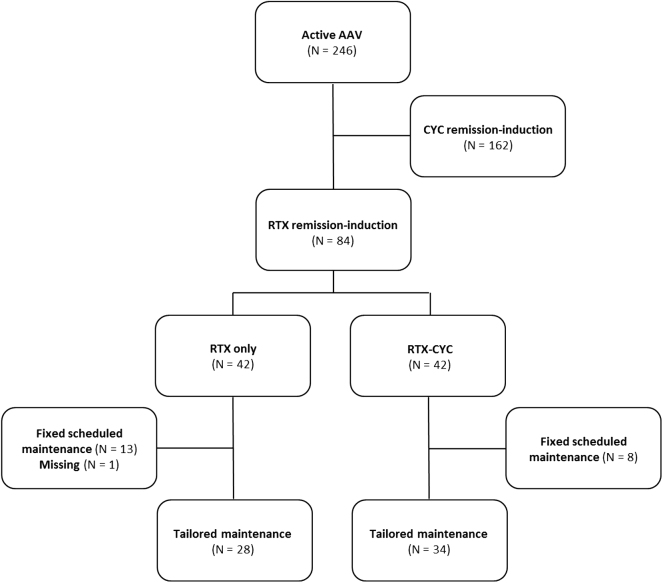
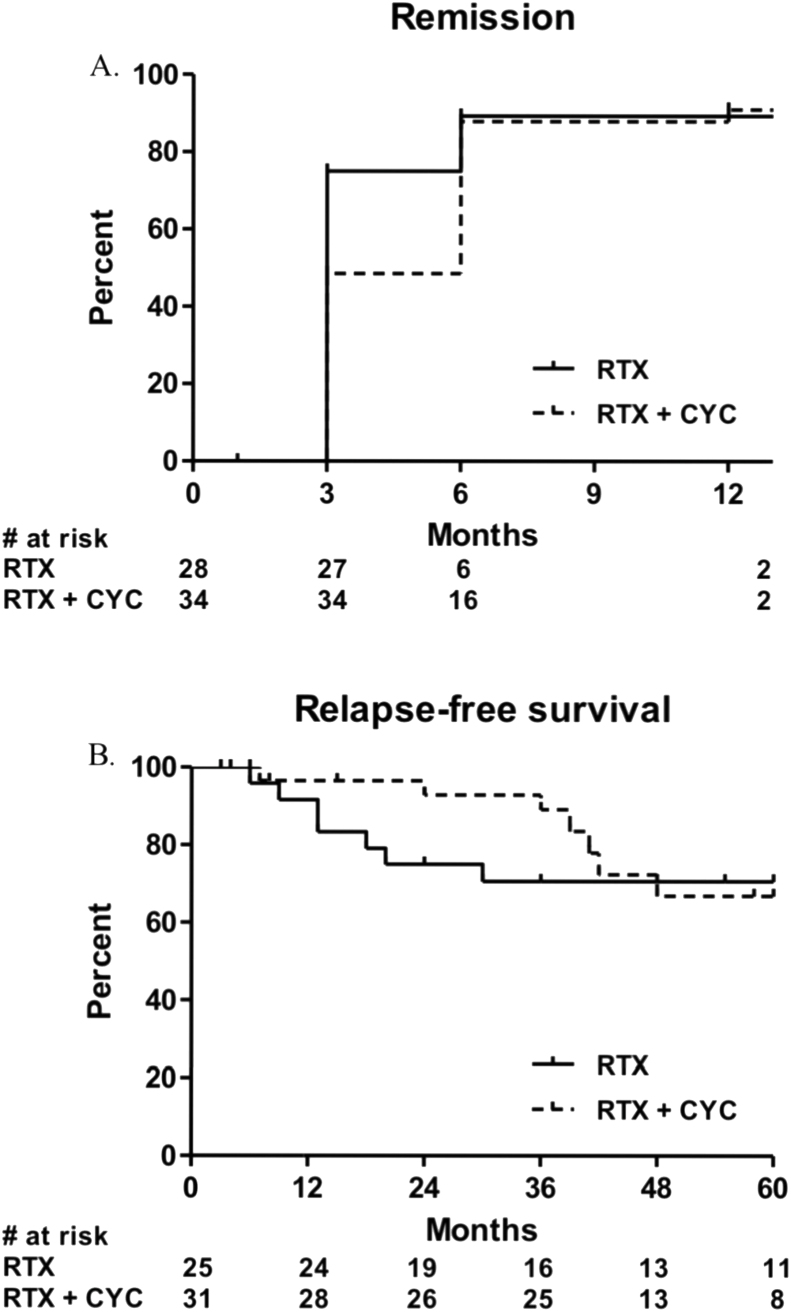
Of the 246 screened patients, 34 received RTX-CYC and 28 RTX only for remission-induction. All patients were followed for at least two years, with a median follow-up of 48 months (IQR 24–60). At baseline, renal involvement was more prevalent in the RTX-CYC patients (85% vs. 61%, P = 0.028). Major relapse rates within two years, but not after five years, were significantly lower in the RTX-CYC group (3% vs. 24%, P = 0.032). The rate of infections, hypogammaglobulinemia, end-stage renal disease, malignancies, and mortality did not differ after two and five years.
Conclusion
Adding low dose CYC to RTX is safe and may prevent major relapses in patients with severe AAV in the first two years after remission-induction. Randomized controlled trials that compare the efficacy and safety between RTX and a combination of RTX with CYC are needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


