Angela B Snyder, Sangeetha Lakshmanan, Mary M Hulihan, Susan T Paulukonis, Mei Zhou, Sophia S Horiuchi, Karon Abe, Shammara N Pope, Laura A Schieve
{"title":"Surveillance for Sickle Cell Disease - Sickle Cell Data Collection Program, Two States, 2004-2018.","authors":"Angela B Snyder, Sangeetha Lakshmanan, Mary M Hulihan, Susan T Paulukonis, Mei Zhou, Sophia S Horiuchi, Karon Abe, Shammara N Pope, Laura A Schieve","doi":"10.15585/mmwr.ss7109a1","DOIUrl":null,"url":null,"abstract":"<p><strong>Problem/condition: </strong>Sickle cell disease (SCD), an inherited blood disorder affecting an estimated 100,000 persons in the United States, is associated with multiple complications and reduced life expectancy. Complications of SCD can include anemia, debilitating acute and chronic pain, infection, acute chest syndrome, stroke, and progressive organ damage, including decreased cognitive function and renal failure. Early diagnosis, screenings and preventive interventions, and access to specialist health care can decrease illness and death. Population-based public health surveillance is critical to understanding the course and outcomes of SCD as well as the health care use, unmet health care needs, and gaps in essential services of the population affected by SCD.</p><p><strong>Period covered: </strong>2004-2018.</p><p><strong>Description of the program: </strong>In 2015, CDC established the Sickle Cell Data Collection (SCDC) program to characterize the epidemiology of SCD in two states (California and Georgia). Previously, surveillance for SCD was conducted by two short-term projects: Registry and Surveillance System for Hemoglobinopathies (RuSH), which was conducted during 2010-2012 and included 2004-2008 data, and Public Health Research, Epidemiology, and Surveillance for Hemoglobinopathies (PHRESH), which was conducted during 2012-2014 and included 2004-2008 data. Both California and Georgia participated in RuSH and PHRESH, which guided the development of the SCDC methods and case definitions. SCDC is a population-based tracking system that uses comprehensive data linkages in state health systems. These linkages serve to synthesize and disseminate population-based, longitudinal data for persons identified with SCD from multiple sources using selected International Classification of Diseases, Ninth Revision, Clinical Modification, and Tenth Revision codes and laboratory results confirmed through state newborn screening (NBS) programs or clinic case reporting. Administrative and clinical data sources include state Medicaid and Children's Health Insurance Program databases, death certificates, NBS programs, hospital discharge and emergency department records, and clinical records or case reports. Data from multiple sources and years are linked and deduplicated so that states can analyze and report on SCD population prevalence, demographic characteristics, health care access and use, and health outcomes. The SCD case definition is based on an algorithm that classifies cases with laboratory confirmation as confirmed cases and those with a reported clinical diagnosis or three or more diagnostic codes over a 5-year period from an administrative data source as probable cases. In 2019, nine states (Alabama, California, Georgia, Indiana, Michigan, Minnesota, North Carolina, Tennessee, and Virginia) were funded as part of an SCDC capacity-building initiative. The newly funded states developed strategies for SCD case identification and data linkage similar to those used by California and Georgia. As of 2021, the SCDC program had expanded to 11 states with the addition of Colorado and Wisconsin.</p><p><strong>Results: </strong>During 2004-2018, the cumulative prevalence of confirmed and probable SCD cases identified in California and Georgia was 9,875 and 14,777 cases, respectively. The 2018 annual prevalence count was 6,027 cases for California and 9,141 for Georgia. Examination of prevalence counts by contributing data source during 2014-2018 revealed that each data source captured 16%-71% of cases in California and 17%-87% in Georgia; therefore, no individual source is sufficient to estimate statewide population prevalence. The proportion of pediatric SCD patients (children aged 0-18 years) was 27% in California and 40% in Georgia. The percentage of females with SCD in California and Georgia was 58% and 57%, respectively. Of the cases with SCD genotyping data available (n = 5,856), 63% of patients had sickle cell anemia. SCDC data have been used to directly apprise health care providers and policymakers about health care needs and gaps for patients with SCD. For example, an SCDC Georgia assessment indicated that 10% of babies born during 2004-2016 with SCD lived more than a 1-hour drive from any SCD specialty care option, and another 14% lived within a 1-hour drive of a periodic SCD specialty clinic only. Likewise, an SCDC California assessment indicated that during 2016-2018, most patients with SCD in Los Angeles County lived approximately 15-60 miles from hematologists experienced in SCD care. A surveillance capacity and performance assessment of all 11 SCDC states during 2020-2021 indicated that states differed in the availability of data sources used for SCD surveillance and the time frames for accessing each state data source. Nonetheless, methods for standardizing reporting were developed across all participating states.</p><p><strong>Interpretation: </strong>This report is the first comprehensive description of CDC's efforts in collaboration with participating states to establish, maintain, and expand SCD surveillance through the SCDC program to improve health outcomes for persons living with SCD. Findings from California and Georgia analyses highlighted a need for additional SCD specialty clinics. Despite different approaches, expansion of SCDC to multiple states was possible using standardized, rigorous methods developed across all participating states for reporting on disease prevalence, health care needs and use, and deaths.</p><p><strong>Public health action: </strong>Findings from surveillance can be used to improve and monitor care and outcomes for persons with SCD. These and other SCDC analyses have had a role in opening new SCD clinics, educating health care providers, developing state health care policies, and guiding new research initiatives. Public health officials can use this report as a guiding framework to plan or implement surveillance programs for persons with SCD. Both data-related activities (data sources; patient identifiers; and obtaining, transferring, and linking data) and the administrative considerations (stakeholder engagement, costs and resources, and long-term sustainability) are crucial to the success of these programs.</p>","PeriodicalId":48549,"journal":{"name":"Mmwr Surveillance Summaries","volume":"71 9","pages":"1-18"},"PeriodicalIF":49.8000,"publicationDate":"2022-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9552568/pdf/","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mmwr Surveillance Summaries","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.15585/mmwr.ss7109a1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 4
Abstract
Problem/condition: Sickle cell disease (SCD), an inherited blood disorder affecting an estimated 100,000 persons in the United States, is associated with multiple complications and reduced life expectancy. Complications of SCD can include anemia, debilitating acute and chronic pain, infection, acute chest syndrome, stroke, and progressive organ damage, including decreased cognitive function and renal failure. Early diagnosis, screenings and preventive interventions, and access to specialist health care can decrease illness and death. Population-based public health surveillance is critical to understanding the course and outcomes of SCD as well as the health care use, unmet health care needs, and gaps in essential services of the population affected by SCD.
Period covered: 2004-2018.
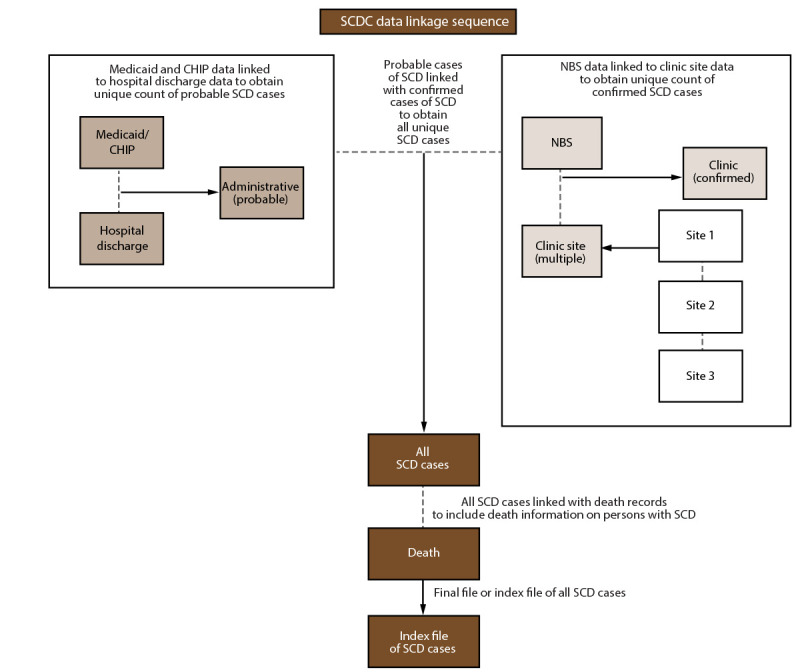
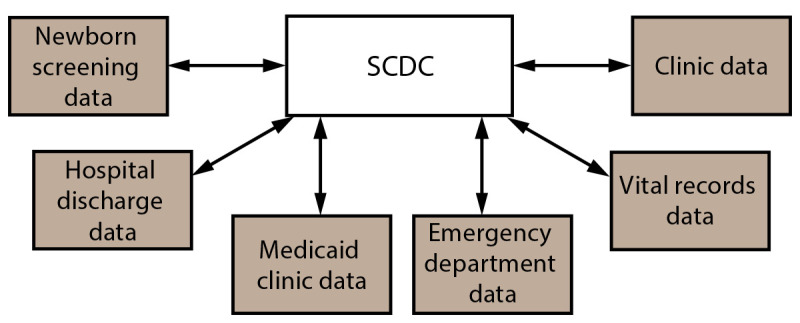
Description of the program: In 2015, CDC established the Sickle Cell Data Collection (SCDC) program to characterize the epidemiology of SCD in two states (California and Georgia). Previously, surveillance for SCD was conducted by two short-term projects: Registry and Surveillance System for Hemoglobinopathies (RuSH), which was conducted during 2010-2012 and included 2004-2008 data, and Public Health Research, Epidemiology, and Surveillance for Hemoglobinopathies (PHRESH), which was conducted during 2012-2014 and included 2004-2008 data. Both California and Georgia participated in RuSH and PHRESH, which guided the development of the SCDC methods and case definitions. SCDC is a population-based tracking system that uses comprehensive data linkages in state health systems. These linkages serve to synthesize and disseminate population-based, longitudinal data for persons identified with SCD from multiple sources using selected International Classification of Diseases, Ninth Revision, Clinical Modification, and Tenth Revision codes and laboratory results confirmed through state newborn screening (NBS) programs or clinic case reporting. Administrative and clinical data sources include state Medicaid and Children's Health Insurance Program databases, death certificates, NBS programs, hospital discharge and emergency department records, and clinical records or case reports. Data from multiple sources and years are linked and deduplicated so that states can analyze and report on SCD population prevalence, demographic characteristics, health care access and use, and health outcomes. The SCD case definition is based on an algorithm that classifies cases with laboratory confirmation as confirmed cases and those with a reported clinical diagnosis or three or more diagnostic codes over a 5-year period from an administrative data source as probable cases. In 2019, nine states (Alabama, California, Georgia, Indiana, Michigan, Minnesota, North Carolina, Tennessee, and Virginia) were funded as part of an SCDC capacity-building initiative. The newly funded states developed strategies for SCD case identification and data linkage similar to those used by California and Georgia. As of 2021, the SCDC program had expanded to 11 states with the addition of Colorado and Wisconsin.
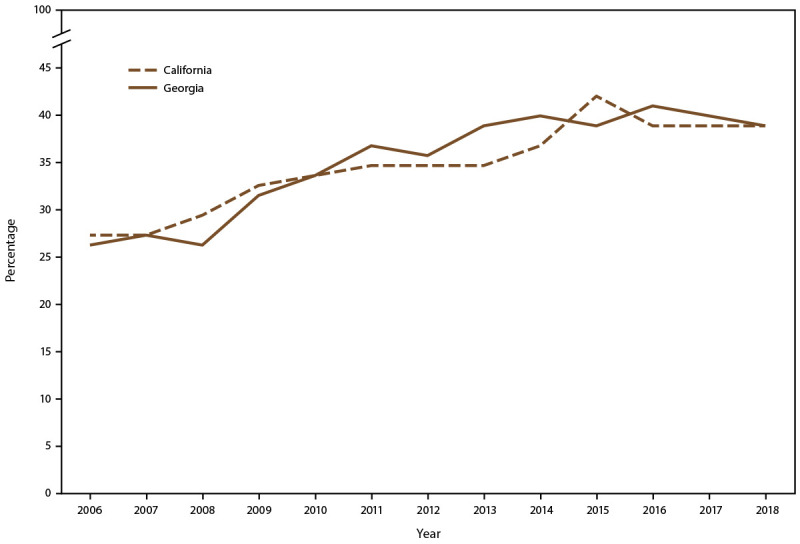
Results: During 2004-2018, the cumulative prevalence of confirmed and probable SCD cases identified in California and Georgia was 9,875 and 14,777 cases, respectively. The 2018 annual prevalence count was 6,027 cases for California and 9,141 for Georgia. Examination of prevalence counts by contributing data source during 2014-2018 revealed that each data source captured 16%-71% of cases in California and 17%-87% in Georgia; therefore, no individual source is sufficient to estimate statewide population prevalence. The proportion of pediatric SCD patients (children aged 0-18 years) was 27% in California and 40% in Georgia. The percentage of females with SCD in California and Georgia was 58% and 57%, respectively. Of the cases with SCD genotyping data available (n = 5,856), 63% of patients had sickle cell anemia. SCDC data have been used to directly apprise health care providers and policymakers about health care needs and gaps for patients with SCD. For example, an SCDC Georgia assessment indicated that 10% of babies born during 2004-2016 with SCD lived more than a 1-hour drive from any SCD specialty care option, and another 14% lived within a 1-hour drive of a periodic SCD specialty clinic only. Likewise, an SCDC California assessment indicated that during 2016-2018, most patients with SCD in Los Angeles County lived approximately 15-60 miles from hematologists experienced in SCD care. A surveillance capacity and performance assessment of all 11 SCDC states during 2020-2021 indicated that states differed in the availability of data sources used for SCD surveillance and the time frames for accessing each state data source. Nonetheless, methods for standardizing reporting were developed across all participating states.
Interpretation: This report is the first comprehensive description of CDC's efforts in collaboration with participating states to establish, maintain, and expand SCD surveillance through the SCDC program to improve health outcomes for persons living with SCD. Findings from California and Georgia analyses highlighted a need for additional SCD specialty clinics. Despite different approaches, expansion of SCDC to multiple states was possible using standardized, rigorous methods developed across all participating states for reporting on disease prevalence, health care needs and use, and deaths.
Public health action: Findings from surveillance can be used to improve and monitor care and outcomes for persons with SCD. These and other SCDC analyses have had a role in opening new SCD clinics, educating health care providers, developing state health care policies, and guiding new research initiatives. Public health officials can use this report as a guiding framework to plan or implement surveillance programs for persons with SCD. Both data-related activities (data sources; patient identifiers; and obtaining, transferring, and linking data) and the administrative considerations (stakeholder engagement, costs and resources, and long-term sustainability) are crucial to the success of these programs.
期刊介绍:
The Morbidity and Mortality Weekly Report (MMWR) Series, produced by the Centers for Disease Control and Prevention (CDC), is commonly referred to as "the voice of CDC." Serving as the primary outlet for timely, reliable, authoritative, accurate, objective, and practical public health information and recommendations, the MMWR is a crucial publication. Its readership primarily includes physicians, nurses, public health practitioners, epidemiologists, scientists, researchers, educators, and laboratorians.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


