Alan C Kwan, Gerran Salto, Trevor-Trung Nguyen, Elizabeth H Kim, Eric Luong, Pranoti Hiremath, David Ouyang, Joseph E Ebinger, Debiao Li, Daniel S Berman, Michelle M Kittleson, Jon A Kobashigawa, Jignesh K Patel, Susan Cheng
{"title":"Cardiac microstructural alterations in immune-inflammatory myocardial disease: a retrospective case-control study.","authors":"Alan C Kwan, Gerran Salto, Trevor-Trung Nguyen, Elizabeth H Kim, Eric Luong, Pranoti Hiremath, David Ouyang, Joseph E Ebinger, Debiao Li, Daniel S Berman, Michelle M Kittleson, Jon A Kobashigawa, Jignesh K Patel, Susan Cheng","doi":"10.1186/s12947-022-00279-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Immune-inflammatory myocardial disease contributes to multiple chronic cardiac processes, but access to non-invasive screening is limited. We have previously developed a method of echocardiographic texture analysis, called the high-spectrum signal intensity coefficient (HS-SIC) which assesses myocardial microstructure and previously associated with myocardial fibrosis. We aimed to determine whether this echocardiographic texture analysis of cardiac microstructure can identify inflammatory cardiac disease in the clinical setting.</p><p><strong>Methods: </strong>We conducted a retrospective case-control study of 318 patients with distinct clinical myocardial pathologies and 20 healthy controls. Populations included myocarditis, atypical chest pain/palpitations, STEMI, severe aortic stenosis, acute COVID infection, amyloidosis, and cardiac transplantation with acute rejection, without current rejection but with prior rejection, and with no history of rejection. We assessed the HS-SIC's ability to differentiate between a broader diversity of clinical groups and healthy controls. We used Kruskal-Wallis tests to compare HS-SIC values measured in each of the clinical populations with those in the healthy control group and compared HS-SIC values between the subgroups of cardiac transplantation rejection status.</p><p><strong>Results: </strong>For the total sample of N = 338, the mean age was 49.6 ± 20.9 years and 50% were women. The mean ± standard error of the mean of HS-SIC were: 0.668 ± 0.074 for controls, 0.552 ± 0.049 for atypical chest pain/palpitations, 0.425 ± 0.058 for myocarditis, 0.881 ± 0.129 for STEMI, 1.116 ± 0.196 for severe aortic stenosis, 0.904 ± 0.116 for acute COVID, and 0.698 ± 0.103 for amyloidosis. Among cardiac transplant recipients, HS-SIC values were 0.478 ± 0.999 for active rejection, 0.594 ± 0.091 for prior rejection, and 1.191 ± 0.442 for never rejection. We observed significant differences in HS-SIC between controls and myocarditis (P = 0.0014), active rejection (P = 0.0076), and atypical chest pain or palpitations (P = 0.0014); as well as between transplant patients with active rejection and those without current or prior rejection (P = 0.031).</p><p><strong>Conclusions: </strong>An echocardiographic method can be used to characterize tissue signatures of microstructural changes across a spectrum of cardiac disease including immune-inflammatory conditions.</p>","PeriodicalId":9613,"journal":{"name":"Cardiovascular Ultrasound","volume":"20 1","pages":"9"},"PeriodicalIF":1.6000,"publicationDate":"2022-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8978375/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Ultrasound","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12947-022-00279-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
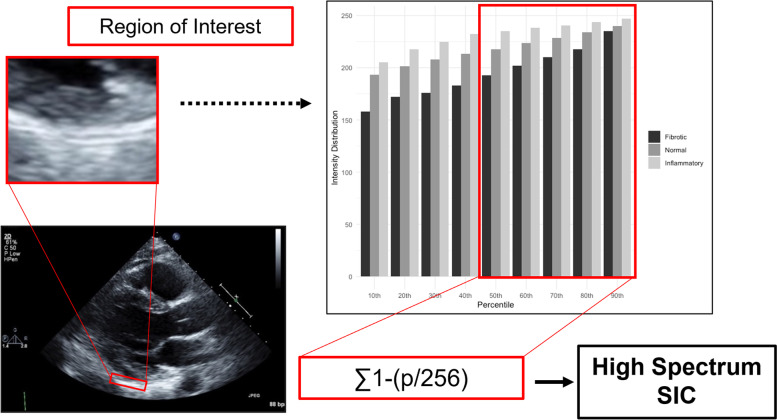
Background: Immune-inflammatory myocardial disease contributes to multiple chronic cardiac processes, but access to non-invasive screening is limited. We have previously developed a method of echocardiographic texture analysis, called the high-spectrum signal intensity coefficient (HS-SIC) which assesses myocardial microstructure and previously associated with myocardial fibrosis. We aimed to determine whether this echocardiographic texture analysis of cardiac microstructure can identify inflammatory cardiac disease in the clinical setting.
Methods: We conducted a retrospective case-control study of 318 patients with distinct clinical myocardial pathologies and 20 healthy controls. Populations included myocarditis, atypical chest pain/palpitations, STEMI, severe aortic stenosis, acute COVID infection, amyloidosis, and cardiac transplantation with acute rejection, without current rejection but with prior rejection, and with no history of rejection. We assessed the HS-SIC's ability to differentiate between a broader diversity of clinical groups and healthy controls. We used Kruskal-Wallis tests to compare HS-SIC values measured in each of the clinical populations with those in the healthy control group and compared HS-SIC values between the subgroups of cardiac transplantation rejection status.
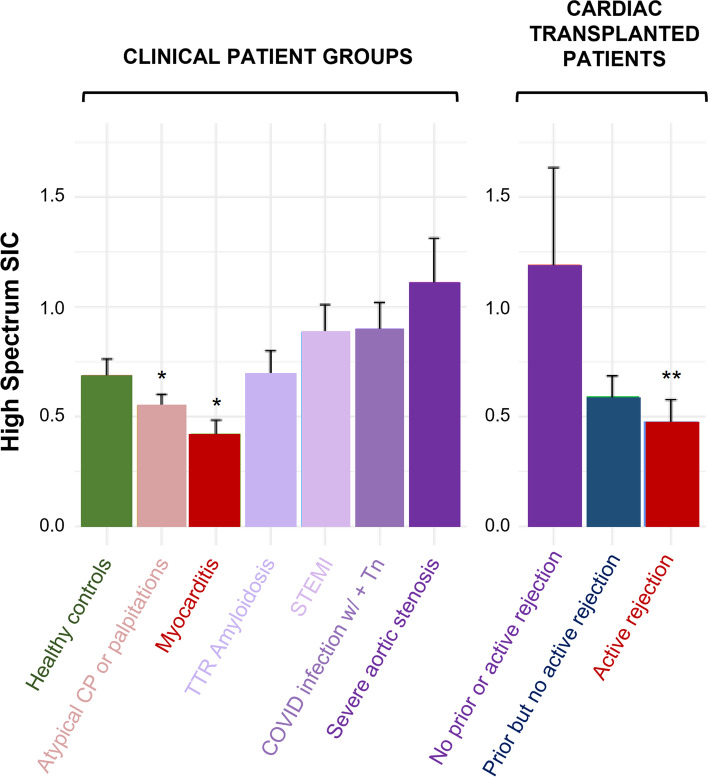
Results: For the total sample of N = 338, the mean age was 49.6 ± 20.9 years and 50% were women. The mean ± standard error of the mean of HS-SIC were: 0.668 ± 0.074 for controls, 0.552 ± 0.049 for atypical chest pain/palpitations, 0.425 ± 0.058 for myocarditis, 0.881 ± 0.129 for STEMI, 1.116 ± 0.196 for severe aortic stenosis, 0.904 ± 0.116 for acute COVID, and 0.698 ± 0.103 for amyloidosis. Among cardiac transplant recipients, HS-SIC values were 0.478 ± 0.999 for active rejection, 0.594 ± 0.091 for prior rejection, and 1.191 ± 0.442 for never rejection. We observed significant differences in HS-SIC between controls and myocarditis (P = 0.0014), active rejection (P = 0.0076), and atypical chest pain or palpitations (P = 0.0014); as well as between transplant patients with active rejection and those without current or prior rejection (P = 0.031).
Conclusions: An echocardiographic method can be used to characterize tissue signatures of microstructural changes across a spectrum of cardiac disease including immune-inflammatory conditions.
期刊介绍:
Cardiovascular Ultrasound is an online journal, publishing peer-reviewed: original research; authoritative reviews; case reports on challenging and/or unusual diagnostic aspects; and expert opinions on new techniques and technologies. We are particularly interested in articles that include relevant images or video files, which provide an additional dimension to published articles and enhance understanding.
As an open access journal, Cardiovascular Ultrasound ensures high visibility for authors in addition to providing an up-to-date and freely available resource for the community. The journal welcomes discussion, and provides a forum for publishing opinion and debate ranging from biology to engineering to clinical echocardiography, with both speed and versatility.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


