Kim Hay Be, Leonardo Zorron Cheng Tao Pu, Brett Pearce, Matthew Lee, Luke Fletcher, Rebecca Cogan, Philip Peyton, Rhys Vaughan, Marios Efthymiou, Sujievvan Chandran
{"title":"High-flow oxygen <i>via</i> oxygenating mouthguard in short upper gastrointestinal endoscopy: A randomised controlled trial.","authors":"Kim Hay Be, Leonardo Zorron Cheng Tao Pu, Brett Pearce, Matthew Lee, Luke Fletcher, Rebecca Cogan, Philip Peyton, Rhys Vaughan, Marios Efthymiou, Sujievvan Chandran","doi":"10.4253/wjge.v14.i12.777","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anaesthetic care during upper gastrointestinal (GI) endoscopy has the unique challenge of maintaining ventilation and oxygenation <i>via</i> a shared upper airway. Supplemental oxygen is recommended by international society guidelines, however, the optimal route or rate of oxygen delivery is not known. Various oxygen delivery devices have been investigated to improve oxygenation during upper GI endoscopy, however, these are limited by commercial availability, costs and in some cases, the expertise required for insertion. Anecdotally at our centre, higher flows of supplemental oxygen can safely be delivered <i>via</i> an oxygenating mouthguard routinely used during upper GI endoscopic procedures.</p><p><strong>Aim: </strong>To assess the incidence of hypoxaemia (SpO<sub>2</sub> < 90%) in patients undergoing upper GI endoscopy receiving supplemental oxygen using an oxygenating mouthguard at 20 L/min flow compared to standard nasal cannula (SNC) at 2 L/min flow.</p><p><strong>Methods: </strong>A single centre, prospective, randomised clinical trial at two sites of an Australian tertiary hospital between October 2020 and September 2021 was conducted. Patients undergoing elective upper gastrointestinal endoscopy under deep sedation were randomised to receive supplemental oxygen <i>via</i> high-flow <i>via</i> oxygenating mouthguard (HFMG) at 20 L/min flow or SNC at 2 L/min flow. The primary outcome was the incidence of hypoxaemia of any duration measured by pulse oximetry. Intraprocedural-related, procedural-related, and sedation-related adverse events and patient-reported outcomes were also recorded.</p><p><strong>Results: </strong>Three hundred patients were randomised. Eight patients were excluded after randomisation. 292 patients were included in the intention-to-treat analysis. The incidence of hypoxaemia was significantly reduced in those allocated HFMG. Six patients (4.4%) allocated to HFMG experienced an episode of hypoxaemia, compared to thirty-four (22.1%) patients allocated to SNC (<i>P</i> value < 0.001). No significant difference was observed in the rates of adverse events or patient-reported outcome measures.</p><p><strong>Conclusion: </strong>The use of HFMG offers a novel approach to reducing the incidence of hypoxaemia during short upper gastrointestinal endoscopic procedures in low-risk patients undergoing deep sedation.</p>","PeriodicalId":23953,"journal":{"name":"World Journal of Gastrointestinal Endoscopy","volume":"14 12","pages":"777-788"},"PeriodicalIF":1.4000,"publicationDate":"2022-12-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/70/a2/WJGE-14-777.PMC9782568.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4253/wjge.v14.i12.777","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
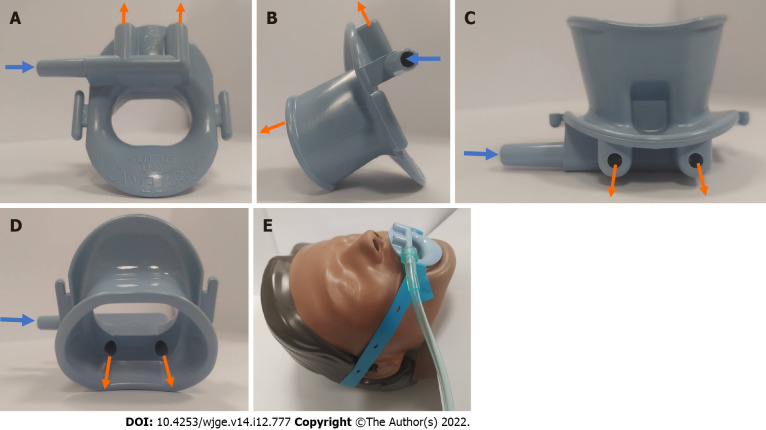
Background: Anaesthetic care during upper gastrointestinal (GI) endoscopy has the unique challenge of maintaining ventilation and oxygenation via a shared upper airway. Supplemental oxygen is recommended by international society guidelines, however, the optimal route or rate of oxygen delivery is not known. Various oxygen delivery devices have been investigated to improve oxygenation during upper GI endoscopy, however, these are limited by commercial availability, costs and in some cases, the expertise required for insertion. Anecdotally at our centre, higher flows of supplemental oxygen can safely be delivered via an oxygenating mouthguard routinely used during upper GI endoscopic procedures.
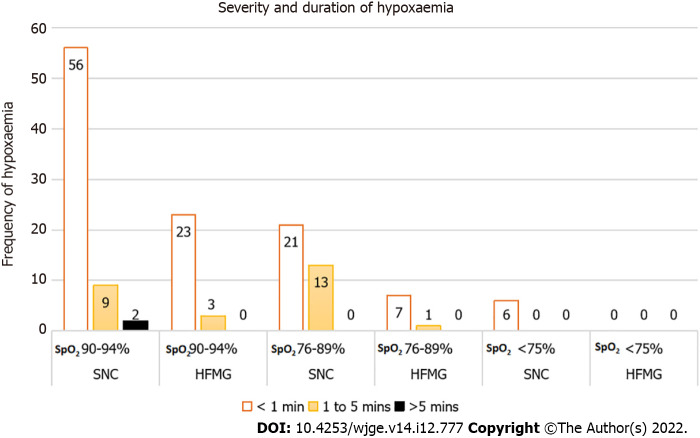
Aim: To assess the incidence of hypoxaemia (SpO2 < 90%) in patients undergoing upper GI endoscopy receiving supplemental oxygen using an oxygenating mouthguard at 20 L/min flow compared to standard nasal cannula (SNC) at 2 L/min flow.
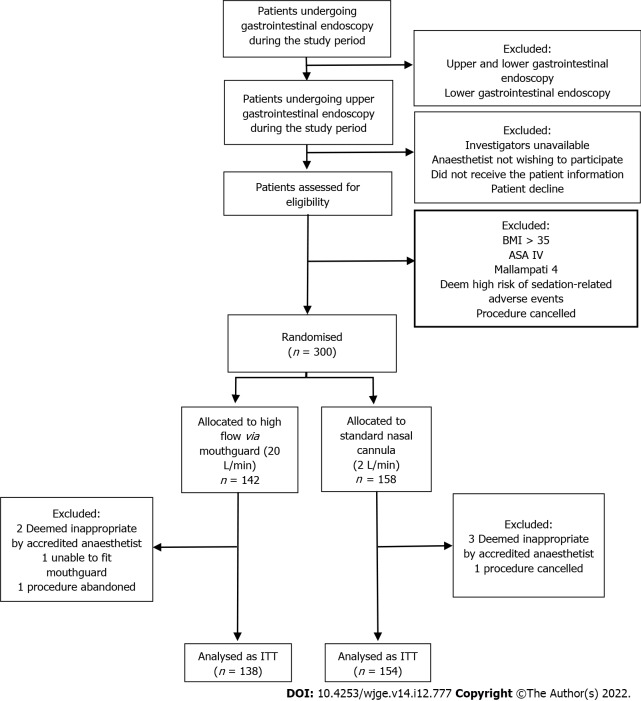
Methods: A single centre, prospective, randomised clinical trial at two sites of an Australian tertiary hospital between October 2020 and September 2021 was conducted. Patients undergoing elective upper gastrointestinal endoscopy under deep sedation were randomised to receive supplemental oxygen via high-flow via oxygenating mouthguard (HFMG) at 20 L/min flow or SNC at 2 L/min flow. The primary outcome was the incidence of hypoxaemia of any duration measured by pulse oximetry. Intraprocedural-related, procedural-related, and sedation-related adverse events and patient-reported outcomes were also recorded.
Results: Three hundred patients were randomised. Eight patients were excluded after randomisation. 292 patients were included in the intention-to-treat analysis. The incidence of hypoxaemia was significantly reduced in those allocated HFMG. Six patients (4.4%) allocated to HFMG experienced an episode of hypoxaemia, compared to thirty-four (22.1%) patients allocated to SNC (P value < 0.001). No significant difference was observed in the rates of adverse events or patient-reported outcome measures.
Conclusion: The use of HFMG offers a novel approach to reducing the incidence of hypoxaemia during short upper gastrointestinal endoscopic procedures in low-risk patients undergoing deep sedation.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


