Nathan Rubalcava, Gabriella A Norwitz, Aimee G Kim, Gary Weiner, Niki Matusko, Meghan A Arnold, George B Mychaliska, Erin E Perrone
{"title":"Neonatal pneumothorax in congenital diaphragmatic hernia: Be wary of high ventilatory pressures.","authors":"Nathan Rubalcava, Gabriella A Norwitz, Aimee G Kim, Gary Weiner, Niki Matusko, Meghan A Arnold, George B Mychaliska, Erin E Perrone","doi":"10.1136/wjps-2021-000341","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with congenital diaphragmatic hernia (CDH) require invasive respiratory support and higher ventilator pressures may be associated with barotrauma. We sought to evaluate the risk factors associated with pneumothorax in CDH neonates prior to repair.</p><p><strong>Methods: </strong>We retrospectively reviewed newborns born with CDH between 2014 and 2019 who developed a pneumothorax, and we matched these cases to patients with CDH without pneumothorax.</p><p><strong>Results: </strong>Twenty-six patients were included (n=13 per group). The pneumothorax group required extracorporeal life support (ECLS) more frequently (85% vs 54%, p=0.04), particularly among type A/B defects (31% vs 7%, p=0.01). The pneumothorax group had higher positive end-expiratory pressure (PEEP) within 1 hour of birth (p=0.02), at pneumothorax diagnosis (p=0.003), and at ECLS (p=0.02). The pneumothorax group had a higher mean airway pressure (Paw) at birth (p=0.01), within 1 hour of birth (p=0.01), and at pneumothorax diagnosis (p=0.04). Using multiple logistic regression with cluster robust SEs, higher Paw (OR 2.2, 95% CI 1.08 to 3.72, p=0.03) and PEEP (OR 1.8, 95% CI 1.15 to 3.14, p=0.007) were associated with an increased risk of developing pneumothorax. There was no difference in survival (p=0.09).</p><p><strong>Conclusions: </strong>Development of a pneumothorax in CDH neonates is independently associated with higher Paw and higher PEEP. A pneumothorax increases the likelihood of treated with ECLS, even with smaller defect.</p>","PeriodicalId":23823,"journal":{"name":"World Journal of Pediatric Surgery","volume":"5 3","pages":"e000341"},"PeriodicalIF":1.3000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b1/d4/wjps-2021-000341.PMC9716795.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Pediatric Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/wjps-2021-000341","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Patients with congenital diaphragmatic hernia (CDH) require invasive respiratory support and higher ventilator pressures may be associated with barotrauma. We sought to evaluate the risk factors associated with pneumothorax in CDH neonates prior to repair.
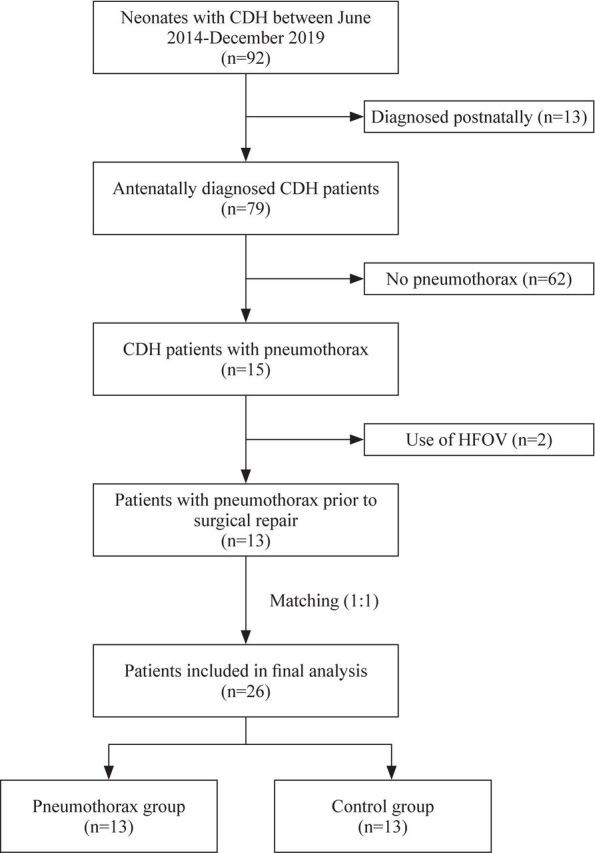
Methods: We retrospectively reviewed newborns born with CDH between 2014 and 2019 who developed a pneumothorax, and we matched these cases to patients with CDH without pneumothorax.
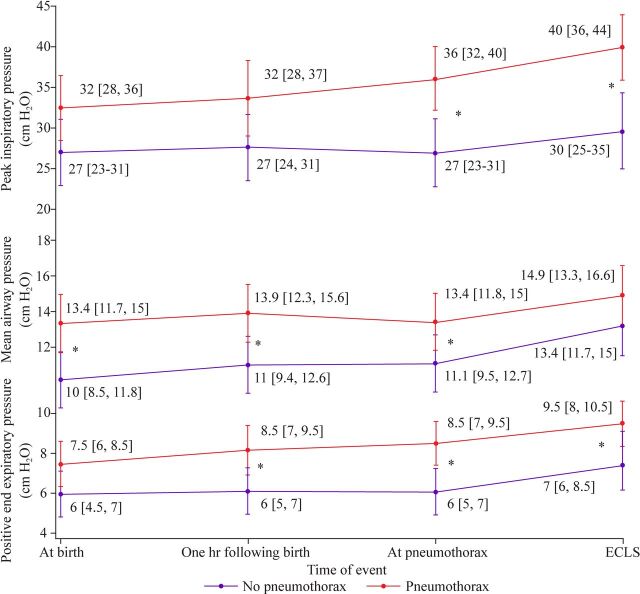
Results: Twenty-six patients were included (n=13 per group). The pneumothorax group required extracorporeal life support (ECLS) more frequently (85% vs 54%, p=0.04), particularly among type A/B defects (31% vs 7%, p=0.01). The pneumothorax group had higher positive end-expiratory pressure (PEEP) within 1 hour of birth (p=0.02), at pneumothorax diagnosis (p=0.003), and at ECLS (p=0.02). The pneumothorax group had a higher mean airway pressure (Paw) at birth (p=0.01), within 1 hour of birth (p=0.01), and at pneumothorax diagnosis (p=0.04). Using multiple logistic regression with cluster robust SEs, higher Paw (OR 2.2, 95% CI 1.08 to 3.72, p=0.03) and PEEP (OR 1.8, 95% CI 1.15 to 3.14, p=0.007) were associated with an increased risk of developing pneumothorax. There was no difference in survival (p=0.09).
Conclusions: Development of a pneumothorax in CDH neonates is independently associated with higher Paw and higher PEEP. A pneumothorax increases the likelihood of treated with ECLS, even with smaller defect.
背景:先天性膈疝(CDH)患者需要有创呼吸支持,较高的呼吸机压力可能与气压创伤有关。我们试图评估修复前与CDH新生儿气胸相关的危险因素。方法:我们回顾性分析了2014年至2019年期间出生的CDH发生气胸的新生儿,并将这些病例与未发生气胸的CDH患者进行了匹配。结果:纳入26例患者(每组13例)。气胸组更频繁地需要体外生命支持(ECLS) (85% vs 54%, p=0.04),特别是A/B型缺陷(31% vs 7%, p=0.01)。气胸组在出生后1小时内(p=0.02)、气胸诊断时(p=0.003)和ECLS时(p=0.02)呼气末正压(PEEP)较高。气胸组在出生时(p=0.01)、出生后1小时内(p=0.01)和气胸诊断时(p=0.04)平均气道压力(Paw)较高。使用具有聚类稳健性se的多元logistic回归,较高的Paw (OR 2.2, 95% CI 1.08至3.72,p=0.03)和PEEP (OR 1.8, 95% CI 1.15至3.14,p=0.007)与气胸发生风险增加相关。两组生存率无差异(p=0.09)。结论:CDH新生儿气胸的发展与较高的Paw和较高的PEEP独立相关。气胸增加了ECLS治疗的可能性,即使是较小的缺损。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


