Fernando Godinho Zampieri, Henrique Palomba, Fernando Augusto Bozza, Daniel C Cubos, Thiago G Romano
{"title":"Acute kidney injury in hospitalized patients with COVID-19: a retrospective cohort.","authors":"Fernando Godinho Zampieri, Henrique Palomba, Fernando Augusto Bozza, Daniel C Cubos, Thiago G Romano","doi":"10.5935/2965-2774.20230428-en","DOIUrl":null,"url":null,"abstract":"Coronavirus disease 2019 (COVID-19) has been reported to cause acute kidney injury (AKI).(1-4) Although severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may directly harm the kidneys through endothelial and coagulation dysfunction,(1) AKI in COVID-19 may also be related to additional organ dysfunctions and other host factors, including mechanical ventilation. The incidence of AKI in hospitalized COVID-19 patients has been suggested to be close to 10.6%, with AKI being strongly associated with increased mortality.(2) We sought to describe the occurrence of AKI in a cohort of hospitalized patients in a private network of hospitals in Brazil during the first COVID wave (March to August 2020). Second, we assessed the interplay between the time of initiation of mechanical ventilation and the occurrence of AKI. Our initial hypothesis was that AKI would predominantly occur after the initiation of mechanical ventilation. The study was approved by the centralized ethics committee with a waiver for consent due to the retrospective nature of its analysis based on anonymized data. We initially selected all 1,602 patients admitted to 45 hospitals in the first wave who had creatinine levels obtained at admission, who did not have a diagnosis of chronic kidney disease, who were older than 18 years old, who had at least one additional creatinine measurement, and who had known hospital outcomes (not transferred to another facility), as shown in figure 1. AKI was defined using two different definitions based on daily information collected up to Fernando Godinho Zampieri1 , Henrique Palomba1 , Fernando Augusto Bozza2 , Daniel C. Cubos1, Thiago G Romano1","PeriodicalId":72721,"journal":{"name":"Critical care science","volume":"35 2","pages":"236-238"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10406411/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5935/2965-2774.20230428-en","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
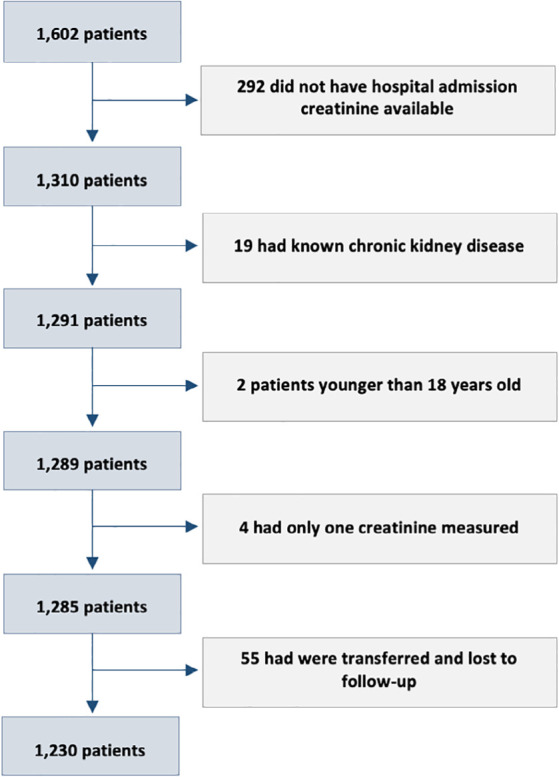
Coronavirus disease 2019 (COVID-19) has been reported to cause acute kidney injury (AKI).(1-4) Although severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may directly harm the kidneys through endothelial and coagulation dysfunction,(1) AKI in COVID-19 may also be related to additional organ dysfunctions and other host factors, including mechanical ventilation. The incidence of AKI in hospitalized COVID-19 patients has been suggested to be close to 10.6%, with AKI being strongly associated with increased mortality.(2) We sought to describe the occurrence of AKI in a cohort of hospitalized patients in a private network of hospitals in Brazil during the first COVID wave (March to August 2020). Second, we assessed the interplay between the time of initiation of mechanical ventilation and the occurrence of AKI. Our initial hypothesis was that AKI would predominantly occur after the initiation of mechanical ventilation. The study was approved by the centralized ethics committee with a waiver for consent due to the retrospective nature of its analysis based on anonymized data. We initially selected all 1,602 patients admitted to 45 hospitals in the first wave who had creatinine levels obtained at admission, who did not have a diagnosis of chronic kidney disease, who were older than 18 years old, who had at least one additional creatinine measurement, and who had known hospital outcomes (not transferred to another facility), as shown in figure 1. AKI was defined using two different definitions based on daily information collected up to Fernando Godinho Zampieri1 , Henrique Palomba1 , Fernando Augusto Bozza2 , Daniel C. Cubos1, Thiago G Romano1

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


