Diana L Pérez-Lozano, Víctor Manuel Camarillo-Nava, Tarsila Elizabeth Juárez-Zepeda, José Elpidio Andrade-Pineda, Danae Pérez-López, Jorge Armando Reyes-Pacheco, Zuley Margarita Lucho-Gutiérrez, Liliana Carmona-Aparicio
{"title":"[Cost-effectiveness of treatment of type 2 diabetes mellitus in México].","authors":"Diana L Pérez-Lozano, Víctor Manuel Camarillo-Nava, Tarsila Elizabeth Juárez-Zepeda, José Elpidio Andrade-Pineda, Danae Pérez-López, Jorge Armando Reyes-Pacheco, Zuley Margarita Lucho-Gutiérrez, Liliana Carmona-Aparicio","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Type 2 Diabetes Mellitus (DM2) is a public health and socioeconomic problem, generating direct medical costs for its treatment.</p><p><strong>Objective: </strong>To analyze the cost-effectiveness of monotherapy and bitherapy treatments in patients with DM2.</p><p><strong>Methods: </strong>Cost-effectiveness, observational, ambispective, cross-sectional and analytical analysis of files in a first level medical unit. The data in the cost matrix was executed with the Office Excel 2010 program; the most prescribed drug was identified and compared with monotherapy and bitherapy.</p><p><strong>Results: </strong>The annual direct medical costs of the total population were drug cost $118,561.70MN, hospitalization cost $243,756.00MN, consultation cost $327,414.00MN and clinical trial cost $2416.79MN, obtaining an annual total of $692,148.58MN. metformin was the most indicated in monotherapy (88.4%) and as standard therapy it has higher cost-effectiveness compared to glibenclamide. In bitherapy it was metformin/glibenclamide (35.7%) versus the therapeutics of metformin/NPH insulin, metformin/insulin glargine and metformin/dapagliflozin, which had a better cost-effective result, with an incremental cost effectiveness of -$1,128,428.50MN, -$34,365.00 MN, -$119,848.97MN respectively.</p><p><strong>Conclusions: </strong>Metformin presented a better cost-effectiveness ratio in monotherapy, while in bitherapy it was the metformin/NPH insulin association.</p>","PeriodicalId":21419,"journal":{"name":"Revista médica del Instituto Mexicano del Seguro Social","volume":"61 2","pages":"172-180"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3a/42/04435117-61-2-172.PMC10396055.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista médica del Instituto Mexicano del Seguro Social","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Type 2 Diabetes Mellitus (DM2) is a public health and socioeconomic problem, generating direct medical costs for its treatment.
Objective: To analyze the cost-effectiveness of monotherapy and bitherapy treatments in patients with DM2.
Methods: Cost-effectiveness, observational, ambispective, cross-sectional and analytical analysis of files in a first level medical unit. The data in the cost matrix was executed with the Office Excel 2010 program; the most prescribed drug was identified and compared with monotherapy and bitherapy.
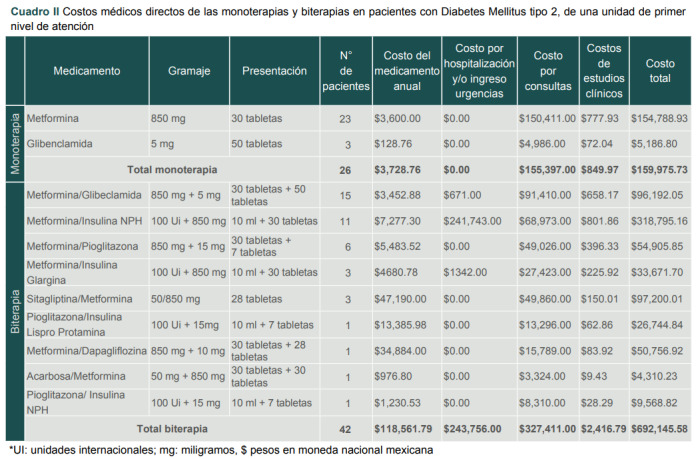
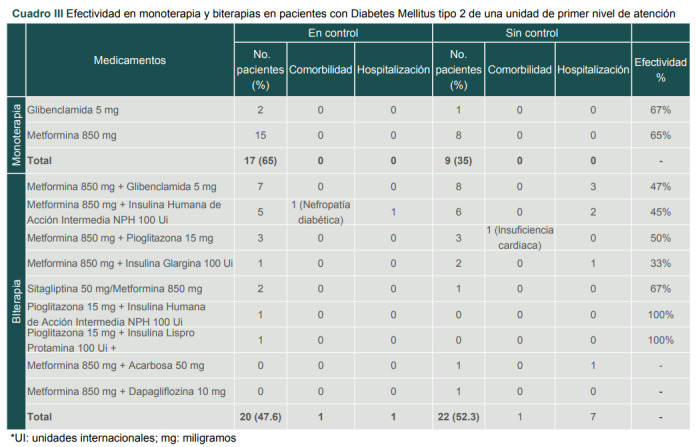
Results: The annual direct medical costs of the total population were drug cost $118,561.70MN, hospitalization cost $243,756.00MN, consultation cost $327,414.00MN and clinical trial cost $2416.79MN, obtaining an annual total of $692,148.58MN. metformin was the most indicated in monotherapy (88.4%) and as standard therapy it has higher cost-effectiveness compared to glibenclamide. In bitherapy it was metformin/glibenclamide (35.7%) versus the therapeutics of metformin/NPH insulin, metformin/insulin glargine and metformin/dapagliflozin, which had a better cost-effective result, with an incremental cost effectiveness of -$1,128,428.50MN, -$34,365.00 MN, -$119,848.97MN respectively.
Conclusions: Metformin presented a better cost-effectiveness ratio in monotherapy, while in bitherapy it was the metformin/NPH insulin association.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


