Changes in pain catastrophizing, fear-avoidance beliefs, and pain self-efficacy mediate changes in pain intensity on disability in the treatment of chronic low back pain.
{"title":"Changes in pain catastrophizing, fear-avoidance beliefs, and pain self-efficacy mediate changes in pain intensity on disability in the treatment of chronic low back pain.","authors":"Truls Ryum, Tore C Stiles","doi":"10.1097/PR9.0000000000001092","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Treatment of chronic low back pain (CLBP) based on the fear-avoidance model (FAM) has received support in randomized controlled trials, but few studies have examined treatment processes associated with treatment outcome. This study examined changes in pain catastrophizing, fear-avoidance beliefs, and pain self-efficacy as mediators of the relation between changes in pain intensity and disability in exposure-based treatment of CLBP.</p><p><strong>Methods: </strong>Data from a randomized controlled trial with 2 treatment arms (exposure treatment based on the FAM with/without in-session exposure) was pooled, including only participants with complete data (N = 69). Change scores (pre to booster session) were computed for all variables, and the indirect effect of change in pain intensity on change in 3 measures of disability, through change in the proposed mediators, was tested in parallel mediation analyses.</p><p><strong>Results: </strong>Decreases in pain catastrophizing and fear-avoidance beliefs, as well as increases in pain self-efficacy, mediated a unique proportion of the relation between changes in pain intensity and disability, depending on the outcome measure. The direct relation between changes in pain intensity and disability was absent when indirect effects were controlled.</p><p><strong>Conclusions: </strong>The results suggest that the way pain is interpreted (pain catastrophizing, fear-avoidance beliefs), as well as pain self-efficacy, are all more critical for reducing disability in exposure-based treatment of CLBP than symptom relief per se.</p>","PeriodicalId":52189,"journal":{"name":"Pain Reports","volume":"8 5","pages":"e1092"},"PeriodicalIF":3.1000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10501475/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pain Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/PR9.0000000000001092","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Treatment of chronic low back pain (CLBP) based on the fear-avoidance model (FAM) has received support in randomized controlled trials, but few studies have examined treatment processes associated with treatment outcome. This study examined changes in pain catastrophizing, fear-avoidance beliefs, and pain self-efficacy as mediators of the relation between changes in pain intensity and disability in exposure-based treatment of CLBP.
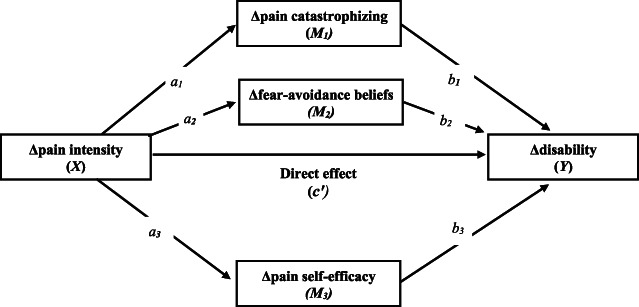
Methods: Data from a randomized controlled trial with 2 treatment arms (exposure treatment based on the FAM with/without in-session exposure) was pooled, including only participants with complete data (N = 69). Change scores (pre to booster session) were computed for all variables, and the indirect effect of change in pain intensity on change in 3 measures of disability, through change in the proposed mediators, was tested in parallel mediation analyses.
Results: Decreases in pain catastrophizing and fear-avoidance beliefs, as well as increases in pain self-efficacy, mediated a unique proportion of the relation between changes in pain intensity and disability, depending on the outcome measure. The direct relation between changes in pain intensity and disability was absent when indirect effects were controlled.
Conclusions: The results suggest that the way pain is interpreted (pain catastrophizing, fear-avoidance beliefs), as well as pain self-efficacy, are all more critical for reducing disability in exposure-based treatment of CLBP than symptom relief per se.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


