Polona Gams, Marko Bitenc, Nenad Danojevic, Tomaz Jensterle, Aleksander Sadikov, Vida Groznik, Maja Sostaric
{"title":"Erector spinae plane block versus intercostal nerve block for postoperative analgesia in lung cancer surgery.","authors":"Polona Gams, Marko Bitenc, Nenad Danojevic, Tomaz Jensterle, Aleksander Sadikov, Vida Groznik, Maja Sostaric","doi":"10.2478/raon-2023-0035","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A recent trend in postoperative analgesia for lung cancer surgery relies on regional nerve blocks with decreased opioid administration. Our study aims to critically assess the continuous ultrasound-guided <i>erector spinae</i> plane block (ESPB) at our institution and compare it to a standard regional anesthetic technique, the intercostal nerve block (ICNB).</p><p><strong>Patients and methods: </strong>A prospective randomized-control study was performed to compare outcomes of patients, scheduled for video-assisted thoracoscopic (VATS) lung cancer resection, allocated to the ESPB or ICNB group. Primary outcomes were total opioid consumption and subjective pain scores at rest and cough each hour in 48 h after surgery. The secondary outcome was respiratory muscle strength, measured by maximal inspiratory and expiratory pressures (MIP/MEP) after 24 h and 48 h.</p><p><strong>Results: </strong>60 patients met the inclusion criteria, half ESPB. Total opioid consumption in the first 48 h was 21. 64 ± 14.22 mg in the ESPB group and 38.34 ± 29.91 mg in the ICNB group (p = 0.035). The patients in the ESPB group had lower numerical rating scores at rest than in the ICNB group (1.19 ± 0.73 <i>vs.</i> 1.77 ± 1.01, p = 0.039). There were no significant differences in MIP/MEP decrease from baseline after 24 h (MIP p = 0.088, MEP p = 0.182) or 48 h (MIP p = 0.110, MEP p = 0.645), time to chest tube removal or hospital discharge between the two groups.</p><p><strong>Conclusions: </strong>In the first 48 h after surgery, patients with continuous ESPB required fewer opioids and reported less pain than patients with ICNB. There were no differences regarding respiratory muscle strength, postoperative complications, and time to hospital discharge. In addition, continuous ESPB demanded more surveillance than ICNB.</p>","PeriodicalId":21034,"journal":{"name":"Radiology and Oncology","volume":"57 3","pages":"364-370"},"PeriodicalIF":2.2000,"publicationDate":"2023-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10476902/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiology and Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2478/raon-2023-0035","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Background: A recent trend in postoperative analgesia for lung cancer surgery relies on regional nerve blocks with decreased opioid administration. Our study aims to critically assess the continuous ultrasound-guided erector spinae plane block (ESPB) at our institution and compare it to a standard regional anesthetic technique, the intercostal nerve block (ICNB).
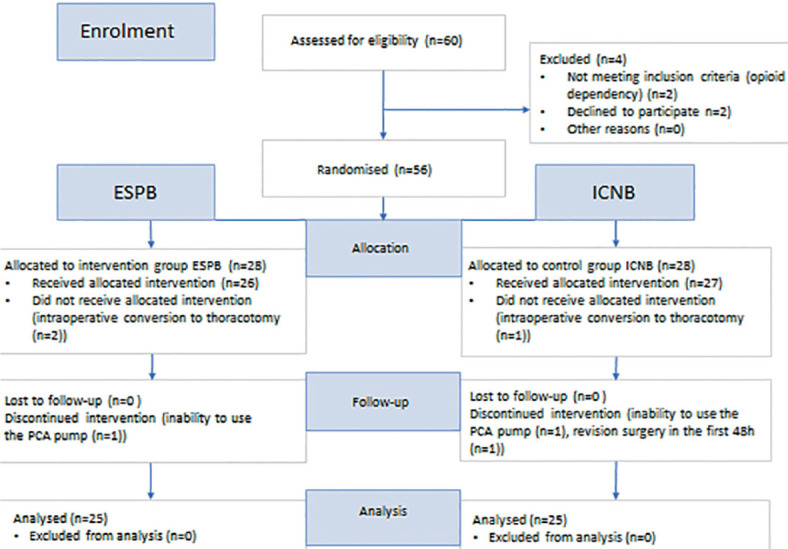
Patients and methods: A prospective randomized-control study was performed to compare outcomes of patients, scheduled for video-assisted thoracoscopic (VATS) lung cancer resection, allocated to the ESPB or ICNB group. Primary outcomes were total opioid consumption and subjective pain scores at rest and cough each hour in 48 h after surgery. The secondary outcome was respiratory muscle strength, measured by maximal inspiratory and expiratory pressures (MIP/MEP) after 24 h and 48 h.
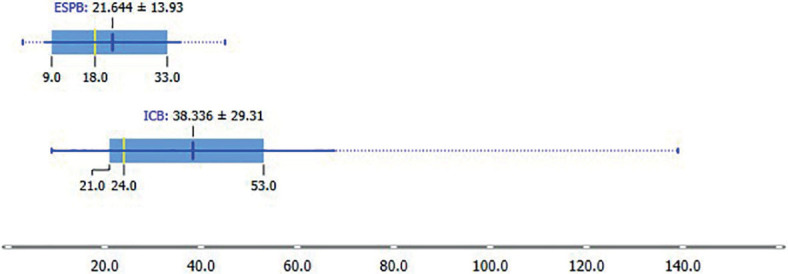
Results: 60 patients met the inclusion criteria, half ESPB. Total opioid consumption in the first 48 h was 21. 64 ± 14.22 mg in the ESPB group and 38.34 ± 29.91 mg in the ICNB group (p = 0.035). The patients in the ESPB group had lower numerical rating scores at rest than in the ICNB group (1.19 ± 0.73 vs. 1.77 ± 1.01, p = 0.039). There were no significant differences in MIP/MEP decrease from baseline after 24 h (MIP p = 0.088, MEP p = 0.182) or 48 h (MIP p = 0.110, MEP p = 0.645), time to chest tube removal or hospital discharge between the two groups.
Conclusions: In the first 48 h after surgery, patients with continuous ESPB required fewer opioids and reported less pain than patients with ICNB. There were no differences regarding respiratory muscle strength, postoperative complications, and time to hospital discharge. In addition, continuous ESPB demanded more surveillance than ICNB.
期刊介绍:
Radiology and Oncology is a multidisciplinary journal devoted to the publishing original and high quality scientific papers and review articles, pertinent to diagnostic and interventional radiology, computerized tomography, magnetic resonance, ultrasound, nuclear medicine, radiotherapy, clinical and experimental oncology, radiobiology, medical physics and radiation protection. Therefore, the scope of the journal is to cover beside radiology the diagnostic and therapeutic aspects in oncology, which distinguishes it from other journals in the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


