Jie Shen, Zhiyuan Wei, Shulin Wang, Xiaohua Wang, Wei Lin, Lei Liu, Guanglin Wang
{"title":"Treatment of infected bone defects with the induced membrane technique.","authors":"Jie Shen, Zhiyuan Wei, Shulin Wang, Xiaohua Wang, Wei Lin, Lei Liu, Guanglin Wang","doi":"10.1302/2046-3758.129.BJR-2022-0439.R2","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>This study aimed to evaluate the effectiveness of the induced membrane technique for treating infected bone defects, and to explore the factors that might affect patient outcomes.</p><p><strong>Methods: </strong>A comprehensive search was performed in PubMed, Embase, and the Cochrane Central Register of Controlled Trials databases between 1 January 2000 and 31 October 2021. Studies with a minimum sample size of five patients with infected bone defects treated with the induced membrane technique were included. Factors associated with nonunion, infection recurrence, and additional procedures were identified using logistic regression analysis on individual patient data.</p><p><strong>Results: </strong>After the screening, 44 studies were included with 1,079 patients and 1,083 segments of infected bone defects treated with the induced membrane technique. The mean defect size was 6.8 cm (0.5 to 30). After the index second stage procedure, 85% (797/942) of segments achieved union, and 92% (999/1,083) of segments achieved final healing. The multivariate analysis with data from 296 patients suggested that older age was associated with higher nonunion risk. Patients with external fixation in the second stage had a significantly higher risk of developing nonunion, increasing the need for additional procedures. The autografts harvested from the femur reamer-irrigator-aspirator increased nonunion, infection recurrence, and additional procedure rates.</p><p><strong>Conclusion: </strong>The induced membrane technique is an effective technique for treating infected bone defects. Internal fixation during the second stage might effectively promote bone healing and reduce additional procedures without increasing infection recurrence. Future studies should standardize individual patient data prospectively to facilitate research on the affected patient outcomes.</p>","PeriodicalId":9074,"journal":{"name":"Bone & Joint Research","volume":"12 9","pages":"546-558"},"PeriodicalIF":4.7000,"publicationDate":"2023-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/76/b7/BJR-12-2046-3758.129.BJR-2022-0439.R2.PMC10495849.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1302/2046-3758.129.BJR-2022-0439.R2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CELL & TISSUE ENGINEERING","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: This study aimed to evaluate the effectiveness of the induced membrane technique for treating infected bone defects, and to explore the factors that might affect patient outcomes.
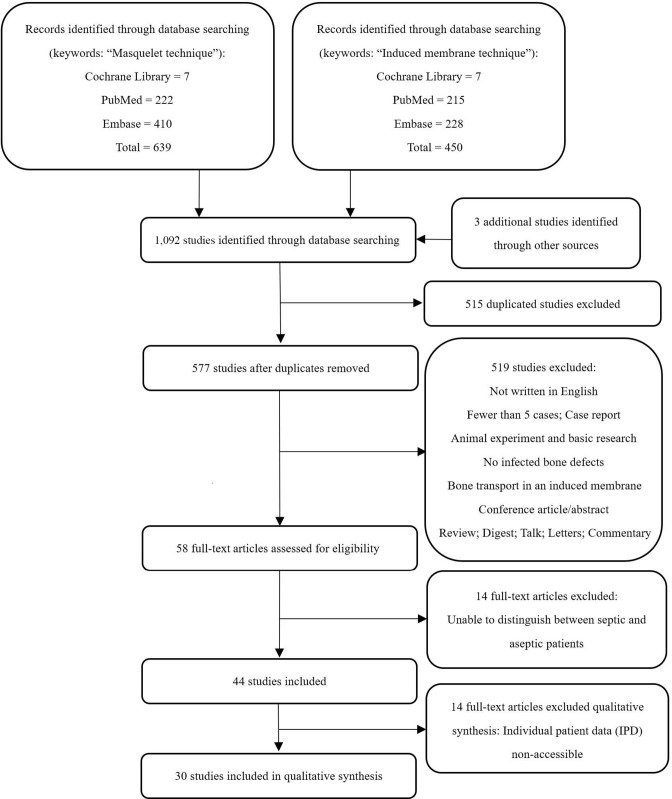
Methods: A comprehensive search was performed in PubMed, Embase, and the Cochrane Central Register of Controlled Trials databases between 1 January 2000 and 31 October 2021. Studies with a minimum sample size of five patients with infected bone defects treated with the induced membrane technique were included. Factors associated with nonunion, infection recurrence, and additional procedures were identified using logistic regression analysis on individual patient data.
Results: After the screening, 44 studies were included with 1,079 patients and 1,083 segments of infected bone defects treated with the induced membrane technique. The mean defect size was 6.8 cm (0.5 to 30). After the index second stage procedure, 85% (797/942) of segments achieved union, and 92% (999/1,083) of segments achieved final healing. The multivariate analysis with data from 296 patients suggested that older age was associated with higher nonunion risk. Patients with external fixation in the second stage had a significantly higher risk of developing nonunion, increasing the need for additional procedures. The autografts harvested from the femur reamer-irrigator-aspirator increased nonunion, infection recurrence, and additional procedure rates.
Conclusion: The induced membrane technique is an effective technique for treating infected bone defects. Internal fixation during the second stage might effectively promote bone healing and reduce additional procedures without increasing infection recurrence. Future studies should standardize individual patient data prospectively to facilitate research on the affected patient outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


