Epidemiology and healthcare utilization of First Nations peoples living with spinal cord injury in Alberta: an observational study to explore health inequities.
Brett F Wegenast, Tara A Whitten, Jeffrey A Bakal, Lea Bill, Adalberto Loyola-Sanchez
{"title":"Epidemiology and healthcare utilization of First Nations peoples living with spinal cord injury in Alberta: an observational study to explore health inequities.","authors":"Brett F Wegenast, Tara A Whitten, Jeffrey A Bakal, Lea Bill, Adalberto Loyola-Sanchez","doi":"10.1038/s41394-023-00603-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>Retrospective observational cohort study.</p><p><strong>Objectives: </strong>Estimate spinal cord injury (SCI) prevalence in First Nations and non-First Nations populations and compare healthcare utilization as an indirect marker of health inequities.</p><p><strong>Setting: </strong>Alberta, Canada.</p><p><strong>Methods: </strong>We created a prevalent adult SCI cohort by identifying cases between April 1, 2002 and December 31, 2017 who were followed for common SCI complications and location of healthcare access from January 1, 2018 to December 31, 2019 using administrative data sources housed within Alberta Health Services (AHS). First Nations and non-First Nations SCI cohorts were divided into SCI etiology: traumatic SCI (TSCI) and non-traumatic SCI (NTSCI). Statistical analyses compared prevalence, demographics, healthcare utilization, and SCI complication rates. A secondary analysis was performed using case matching for demographics, injury type, injury level, and comorbidities.</p><p><strong>Results: </strong>TSCI prevalence: 248 and 117 per 100,000 in First Nations and non-First Nations cohorts, respectively. NTSCI prevalence: 74 and 50 per 100,000 in First Nations and non-First Nations cohorts, respectively. Visit rates were higher in the TSCI First Nations cohort for visits to General Practitioner (GP), Emergency Department (ED), inpatient visits, and inpatient days with higher complication rates due to pulmonary, genitourinary, skin, and 'other' causes after case matching. Visits rates were higher in the NTSCI First Nations cohort for GP and specialists without differences in complication types after case matching.</p><p><strong>Conclusions: </strong>Significant differences exist between First Nations and non-First Nations cohorts living with SCI in Alberta, suggesting healthcare inequities against First Nations Peoples in this province.</p>","PeriodicalId":22079,"journal":{"name":"Spinal Cord Series and Cases","volume":"9 1","pages":"48"},"PeriodicalIF":0.7000,"publicationDate":"2023-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10484972/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spinal Cord Series and Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1038/s41394-023-00603-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study design: Retrospective observational cohort study.
Objectives: Estimate spinal cord injury (SCI) prevalence in First Nations and non-First Nations populations and compare healthcare utilization as an indirect marker of health inequities.
Setting: Alberta, Canada.
Methods: We created a prevalent adult SCI cohort by identifying cases between April 1, 2002 and December 31, 2017 who were followed for common SCI complications and location of healthcare access from January 1, 2018 to December 31, 2019 using administrative data sources housed within Alberta Health Services (AHS). First Nations and non-First Nations SCI cohorts were divided into SCI etiology: traumatic SCI (TSCI) and non-traumatic SCI (NTSCI). Statistical analyses compared prevalence, demographics, healthcare utilization, and SCI complication rates. A secondary analysis was performed using case matching for demographics, injury type, injury level, and comorbidities.
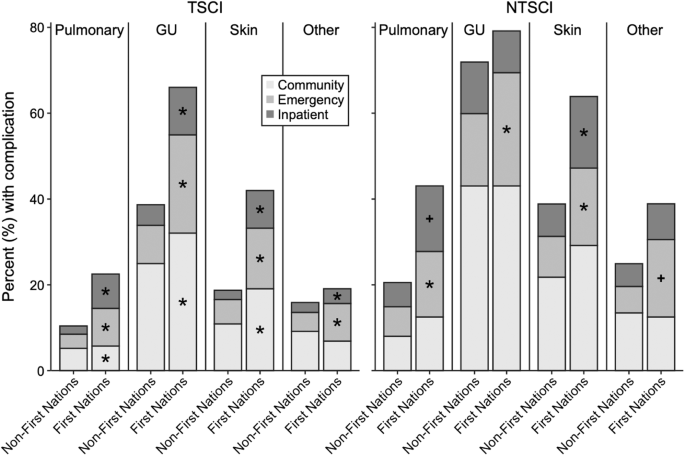
Results: TSCI prevalence: 248 and 117 per 100,000 in First Nations and non-First Nations cohorts, respectively. NTSCI prevalence: 74 and 50 per 100,000 in First Nations and non-First Nations cohorts, respectively. Visit rates were higher in the TSCI First Nations cohort for visits to General Practitioner (GP), Emergency Department (ED), inpatient visits, and inpatient days with higher complication rates due to pulmonary, genitourinary, skin, and 'other' causes after case matching. Visits rates were higher in the NTSCI First Nations cohort for GP and specialists without differences in complication types after case matching.
Conclusions: Significant differences exist between First Nations and non-First Nations cohorts living with SCI in Alberta, suggesting healthcare inequities against First Nations Peoples in this province.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


