Katie Ridge, Helen Fogarty, Dearbhla Doherty, Mary Byrne, Cliona O’Farrelly, James S. O’Donnell, Niall Conlon
{"title":"Enhanced thrombin generation potential and endothelial dysfunction in chronic spontaneous urticaria","authors":"Katie Ridge, Helen Fogarty, Dearbhla Doherty, Mary Byrne, Cliona O’Farrelly, James S. O’Donnell, Niall Conlon","doi":"10.1002/clt2.12285","DOIUrl":null,"url":null,"abstract":"<p>Chronic spontaneous urticaria (CSU) is characterized by recurrent hives that last longer than 6 weeks. The relationship between the coagulation cascade, endothelial cell (EC) activation and urticaria pathogenesis is acknowledged but remains poorly understood.<span><sup>1, 2</sup></span> Examination of these pathways may offer opportunities for improved disease endotyping, prognostication and novel therapeutic avenues.</p><p>Mast cells and eosinophils are known to be important in CSU pathogenesis.<span><sup>3, 4</sup></span> Mast cell degranulation results in the generation of leukotrienes and mast cell-derived mediators. Resulting EC activation promotes vascular permeability. Activated eosinophils express tissue factor, which initiates coagulation via Factor VII.<span><sup>3</sup></span> Despite our understanding of these pathways, the distinct profiles of coagulation and fibrinolysis in CSU remain obscure. Furthermore, products of fibrinolysis, such as D-Dimer, are increasingly proposed as potential markers of severe disease.<span><sup>4</sup></span> This study sought to examine markers of EC activation as well as the dynamics of thrombin generation (TG) in patients with CSU.</p><p>Adult patients with a diagnosis of CSU attending an urticaria clinic at a tertiary Irish teaching Hospital were invited to participate. The study received ethical approval and informed written consent was obtained. Patients (<i>N</i> = 26) with CSU completed the urticaria control test, a measure of disease control assessing hives and swellings over the past 4 weeks.<span><sup>5</sup></span> In this four item questionnaire with scores of 0–16, lower scores indicate higher symptom burden. A healthy control group without a diagnosis of CSU was recruited (<i>N</i> = 18). Markers of EC activation included plasma von Willebrand Factor (VWF) antigen (VWF:Ag) and procoagulant Factor VIII (FVIII:C) levels. These assays, in conjunction with a thrombin generation assay (TGA), were performed on participant plasma as previously described.<span><sup>6</sup></span> Statistical analyses were performed using <i>t</i> tests in GraphPad Prism 9.0 (GraphPad Software) with a <i>p</i> value of < 0.05 considered statistically significant.</p><p>We assessed levels of TG, plasma FVIII:C and plasma VWF:Ag and compared them with levels found in the control group. We also compared patients with CSU who were in receipt of anti-IgE therapy and high dose antihistamines with CSU patients on high dose antihistamines only.</p><p>Baseline characteristics are outlined in Table 1. CSU patients had a distinct TG profile relative to controls with an increased peak thrombin (<i>p</i> ≤ 0.0001) shortened time to peak thrombin (<i>p</i> = 0.004) and an enhanced velocity index (<i>p</i> = 0.0001) (see Figure 1). There was a trend towards elevated endogenous thrombin potential (ETP) in patients with CSU although this was not statistically significant (<i>p</i> = 0.07). Neither age and gender nor the presence of angioedema significantly influenced TG parameters.</p><p>Elevated plasma FVIII:C levels are known to influence TG. We assessed plasma FVIII:C (<i>n</i> = 20). The reference range for FVIII:C is 0.60–1.36 IU/mL. Six of 20 patients with CSU had a FVIII:C level above 1.36 IU/mL. FVIII:C levels correlated with ETP (<i>p</i> < 0.0001), peak thrombin (<i>p</i> < 0.0001), time to peak thrombin (<i>p</i> < 0.0001) and lag time (<i>p</i> < 0.0001), suggesting that increased plasma FVIII:C levels may contribute towards increased TG in patients with CSU.</p><p>To further investigate the elevated FVIII:C seen in some CSU samples, we assessed plasma VWF:Ag (<i>n</i> = 21). The majority of FVIII:C circulates in normal plasma complexed with VWF. Both factors are predominantly synthesized by ECs, and VWF is a marker of acute and chronic endothelial activation.<span><sup>7</sup></span> VWF:Ag levels correlated strongly with FVIII:C levels (<i>r</i> = 0.759, <i>p</i> < 0.001) and seven out of 20 patients with CSU had a VWF:Ag levels above the upper limit of normal (0.50–1.50 IU/mL).</p><p>We compared TG in patients with CSU who were receiving anti-IgE therapy with those who were not. We found that patients who were not receiving anti-IgE therapy had significantly shorter lag times than those who were receiving anti- IgE therapy (<i>p</i> = 0.0264, 95% confidence interval −2.903 to −0.2045). This implies that patients who were on anti-IgE therapy took longer to generate thrombin. A previous study on the effect of anti-IgE therapy on TG in CSU found a significant effect on Factor 1 and Factor 2 with no other significant change in TGA parameters.<span><sup>8</sup></span> Future research may benefit from examining the links between disease control and TG profiles.</p><p>Despite the interpretive constraints of our small sample size, this study identifies for the first time, a relationship between VWF:Ag, FVIII:C and TG in CSU. Elevated plasma VWF has been reported as a marker of EC dysfunction in a range of clinical conditions reflecting acute and chronic endothelial activation.<span><sup>6, 7, 9</sup></span> Our findings point to significantly enhanced TG potential and endothelial dysfunction in CSU. Importantly, VWF and FVIII:C levels correlated strongly with markers of TG, suggesting that EC activation may modulate TG in these patients. Patients with CSU do not have a reported increased clotting risk. Nevertheless, our data demonstrate significantly higher peak thrombin levels in patients with CSU compared to controls. Furthermore, patients who were receiving anti-IgE therapy at the time of sampling had longer lag times, indicating that anti-IgE therapy affects thrombin lagtime.</p><p>Plasma FVIII:C may be an important part of the inflammatory signal in CSU. Further interrogation of this parameter in CSU may improve our understanding of crosstalk between immune cell activation and the coagulation cascade. We propose that the TGA is a key tool for probing the complexities of coagulation and fibrinolysis in this cohort of patients. Further studies on biomarkers of endothelial dysfunction may help identify disease subgroups that could benefit from the manipulation of the coagulation system.</p><p>Niall Conlon, Cliona O’Farrelly and James S. O’Donnell conceived the research plan. Helen Fogarty, Dearbhla Doherty and Mary Byrne performed laboratory experiments. Katie Ridge performed statistical analysis and wrote the manuscript. All authors reviewed and critiqued the final manuscript.</p><p>The authors whose names are listed immediately below certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.</p><p>Wellcome Trust and the Health Research Board, Grant/Award Number: 203930/B/16/Z; Health Service Executive, National Doctors Training and Planning; Health and Social Care, Research and Development Division, Northern Ireland.</p>","PeriodicalId":10334,"journal":{"name":"Clinical and Translational Allergy","volume":null,"pages":null},"PeriodicalIF":4.6000,"publicationDate":"2023-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clt2.12285","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clt2.12285","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Chronic spontaneous urticaria (CSU) is characterized by recurrent hives that last longer than 6 weeks. The relationship between the coagulation cascade, endothelial cell (EC) activation and urticaria pathogenesis is acknowledged but remains poorly understood.1, 2 Examination of these pathways may offer opportunities for improved disease endotyping, prognostication and novel therapeutic avenues.
Mast cells and eosinophils are known to be important in CSU pathogenesis.3, 4 Mast cell degranulation results in the generation of leukotrienes and mast cell-derived mediators. Resulting EC activation promotes vascular permeability. Activated eosinophils express tissue factor, which initiates coagulation via Factor VII.3 Despite our understanding of these pathways, the distinct profiles of coagulation and fibrinolysis in CSU remain obscure. Furthermore, products of fibrinolysis, such as D-Dimer, are increasingly proposed as potential markers of severe disease.4 This study sought to examine markers of EC activation as well as the dynamics of thrombin generation (TG) in patients with CSU.
Adult patients with a diagnosis of CSU attending an urticaria clinic at a tertiary Irish teaching Hospital were invited to participate. The study received ethical approval and informed written consent was obtained. Patients (N = 26) with CSU completed the urticaria control test, a measure of disease control assessing hives and swellings over the past 4 weeks.5 In this four item questionnaire with scores of 0–16, lower scores indicate higher symptom burden. A healthy control group without a diagnosis of CSU was recruited (N = 18). Markers of EC activation included plasma von Willebrand Factor (VWF) antigen (VWF:Ag) and procoagulant Factor VIII (FVIII:C) levels. These assays, in conjunction with a thrombin generation assay (TGA), were performed on participant plasma as previously described.6 Statistical analyses were performed using t tests in GraphPad Prism 9.0 (GraphPad Software) with a p value of < 0.05 considered statistically significant.
We assessed levels of TG, plasma FVIII:C and plasma VWF:Ag and compared them with levels found in the control group. We also compared patients with CSU who were in receipt of anti-IgE therapy and high dose antihistamines with CSU patients on high dose antihistamines only.
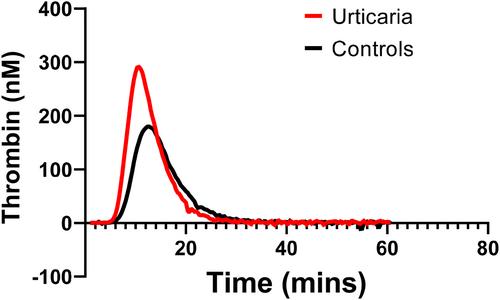
Baseline characteristics are outlined in Table 1. CSU patients had a distinct TG profile relative to controls with an increased peak thrombin (p ≤ 0.0001) shortened time to peak thrombin (p = 0.004) and an enhanced velocity index (p = 0.0001) (see Figure 1). There was a trend towards elevated endogenous thrombin potential (ETP) in patients with CSU although this was not statistically significant (p = 0.07). Neither age and gender nor the presence of angioedema significantly influenced TG parameters.
Elevated plasma FVIII:C levels are known to influence TG. We assessed plasma FVIII:C (n = 20). The reference range for FVIII:C is 0.60–1.36 IU/mL. Six of 20 patients with CSU had a FVIII:C level above 1.36 IU/mL. FVIII:C levels correlated with ETP (p < 0.0001), peak thrombin (p < 0.0001), time to peak thrombin (p < 0.0001) and lag time (p < 0.0001), suggesting that increased plasma FVIII:C levels may contribute towards increased TG in patients with CSU.
To further investigate the elevated FVIII:C seen in some CSU samples, we assessed plasma VWF:Ag (n = 21). The majority of FVIII:C circulates in normal plasma complexed with VWF. Both factors are predominantly synthesized by ECs, and VWF is a marker of acute and chronic endothelial activation.7 VWF:Ag levels correlated strongly with FVIII:C levels (r = 0.759, p < 0.001) and seven out of 20 patients with CSU had a VWF:Ag levels above the upper limit of normal (0.50–1.50 IU/mL).
We compared TG in patients with CSU who were receiving anti-IgE therapy with those who were not. We found that patients who were not receiving anti-IgE therapy had significantly shorter lag times than those who were receiving anti- IgE therapy (p = 0.0264, 95% confidence interval −2.903 to −0.2045). This implies that patients who were on anti-IgE therapy took longer to generate thrombin. A previous study on the effect of anti-IgE therapy on TG in CSU found a significant effect on Factor 1 and Factor 2 with no other significant change in TGA parameters.8 Future research may benefit from examining the links between disease control and TG profiles.
Despite the interpretive constraints of our small sample size, this study identifies for the first time, a relationship between VWF:Ag, FVIII:C and TG in CSU. Elevated plasma VWF has been reported as a marker of EC dysfunction in a range of clinical conditions reflecting acute and chronic endothelial activation.6, 7, 9 Our findings point to significantly enhanced TG potential and endothelial dysfunction in CSU. Importantly, VWF and FVIII:C levels correlated strongly with markers of TG, suggesting that EC activation may modulate TG in these patients. Patients with CSU do not have a reported increased clotting risk. Nevertheless, our data demonstrate significantly higher peak thrombin levels in patients with CSU compared to controls. Furthermore, patients who were receiving anti-IgE therapy at the time of sampling had longer lag times, indicating that anti-IgE therapy affects thrombin lagtime.
Plasma FVIII:C may be an important part of the inflammatory signal in CSU. Further interrogation of this parameter in CSU may improve our understanding of crosstalk between immune cell activation and the coagulation cascade. We propose that the TGA is a key tool for probing the complexities of coagulation and fibrinolysis in this cohort of patients. Further studies on biomarkers of endothelial dysfunction may help identify disease subgroups that could benefit from the manipulation of the coagulation system.
Niall Conlon, Cliona O’Farrelly and James S. O’Donnell conceived the research plan. Helen Fogarty, Dearbhla Doherty and Mary Byrne performed laboratory experiments. Katie Ridge performed statistical analysis and wrote the manuscript. All authors reviewed and critiqued the final manuscript.
The authors whose names are listed immediately below certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Wellcome Trust and the Health Research Board, Grant/Award Number: 203930/B/16/Z; Health Service Executive, National Doctors Training and Planning; Health and Social Care, Research and Development Division, Northern Ireland.
期刊介绍:
Clinical and Translational Allergy, one of several journals in the portfolio of the European Academy of Allergy and Clinical Immunology, provides a platform for the dissemination of allergy research and reviews, as well as EAACI position papers, task force reports and guidelines, amongst an international scientific audience.
Clinical and Translational Allergy accepts clinical and translational research in the following areas and other related topics: asthma, rhinitis, rhinosinusitis, drug hypersensitivity, allergic conjunctivitis, allergic skin diseases, atopic eczema, urticaria, angioedema, venom hypersensitivity, anaphylaxis, food allergy, immunotherapy, immune modulators and biologics, animal models of allergic disease, immune mechanisms, or any other topic related to allergic disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


