Anne E Palermo, Jane E Butler, Claire L Boswell-Ruys
{"title":"Comparison of two inspiratory muscle training protocols in people with spinal cord injury: a secondary analysis.","authors":"Anne E Palermo, Jane E Butler, Claire L Boswell-Ruys","doi":"10.1038/s41394-023-00594-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design/setting: </strong>Secondary analysis.</p><p><strong>Objectives: </strong>To compare the change in maximal inspiratory pressure (PI<sub>max</sub>) over the first 4 weeks of two different inspiratory muscle training (IMT) protocols and explore if either method is more effective for people with spinal cord injury.</p><p><strong>Methods: </strong>Data originated from two published studies. Participants completed flow-resistive IMT (F-IMT) at 80% daily PI<sub>max,</sub> 7 days/week (supervised weekly), or threshold IMT (T-IMT) at 30-80% weekly PI<sub>max,</sub> twice-daily, 5 days/week (supervised every session). Seven participants from each trial were matched by training adherence, level of spinal cord injury, impairment grade (A-C), and height. Differences between F-IMT and T-IMT groups in training intensity, breaths taken, inspiratory work, and the change in the PI<sub>max</sub> from baseline at the end of week four were analysed.</p><p><strong>Results: </strong>Over 4 weeks, there was no difference in the change in PI<sub>max</sub> between groups (Absolute change in PI<sub>max</sub> (cmH<sub>2</sub>O): p = 0.456, Percent change in PI<sub>max</sub> relative to baseline: p = 0.128). F-IMT participants trained at a higher intensity (median: 77 vs 22 cmH<sub>2</sub>O, p = 0.001 and 80% baseline vs 61% baseline, p = 0.038) but took fewer breaths (840 vs 1404 breaths, p = 0.017) than T-IMT participants. Inspiratory work was similar between groups (64,789 vs 65,910 (% PI<sub>max</sub> × number of breaths), p = 0.535).</p><p><strong>Conclusions: </strong>Our findings support both methods of IMT as the change in PI<sub>max</sub> and inspiratory work were similar between groups. However, daily high-intensity F-IMT with intermittent supervision, required fewer breaths and less participant and therapist time. Future studies should examine optimal dosage and supervision required to achieve increased PI<sub>max</sub>.</p>","PeriodicalId":22079,"journal":{"name":"Spinal Cord Series and Cases","volume":"9 1","pages":"42"},"PeriodicalIF":0.9000,"publicationDate":"2023-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10423237/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spinal Cord Series and Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1038/s41394-023-00594-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study design/setting: Secondary analysis.
Objectives: To compare the change in maximal inspiratory pressure (PImax) over the first 4 weeks of two different inspiratory muscle training (IMT) protocols and explore if either method is more effective for people with spinal cord injury.
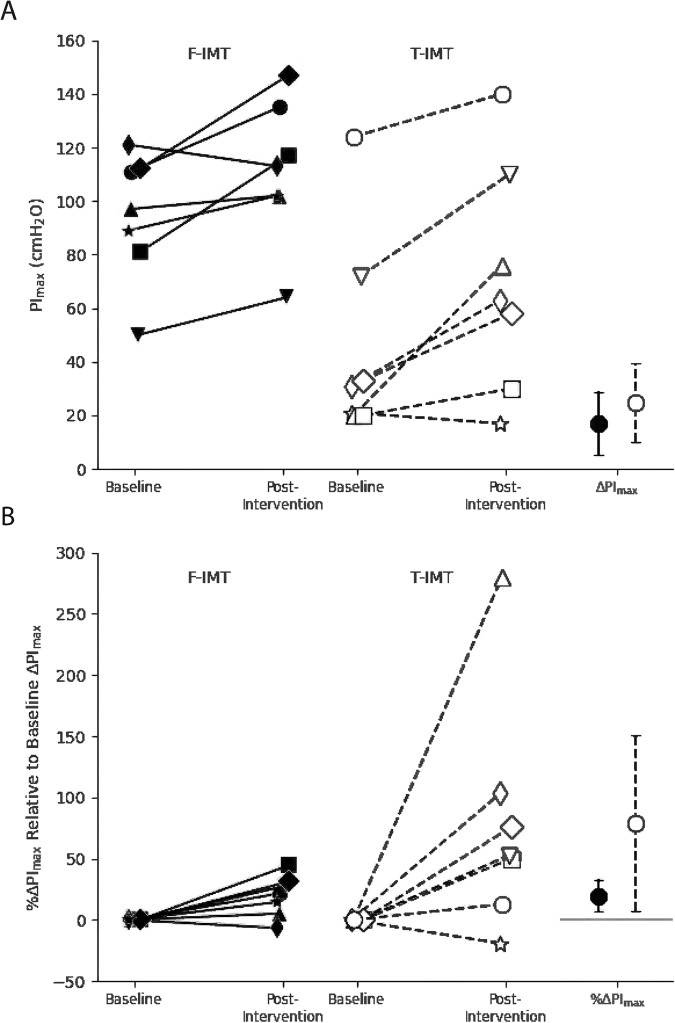
Methods: Data originated from two published studies. Participants completed flow-resistive IMT (F-IMT) at 80% daily PImax, 7 days/week (supervised weekly), or threshold IMT (T-IMT) at 30-80% weekly PImax, twice-daily, 5 days/week (supervised every session). Seven participants from each trial were matched by training adherence, level of spinal cord injury, impairment grade (A-C), and height. Differences between F-IMT and T-IMT groups in training intensity, breaths taken, inspiratory work, and the change in the PImax from baseline at the end of week four were analysed.
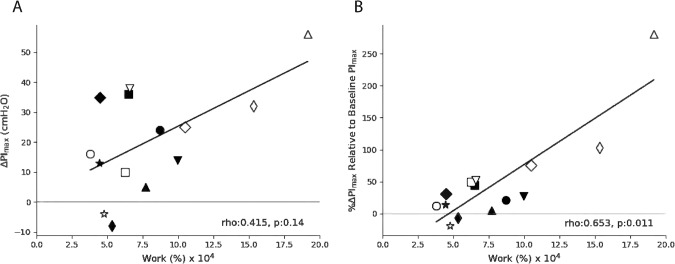
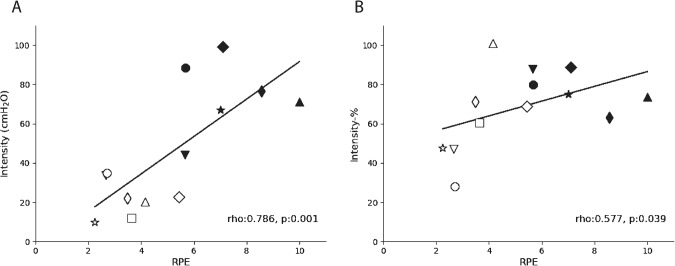
Results: Over 4 weeks, there was no difference in the change in PImax between groups (Absolute change in PImax (cmH2O): p = 0.456, Percent change in PImax relative to baseline: p = 0.128). F-IMT participants trained at a higher intensity (median: 77 vs 22 cmH2O, p = 0.001 and 80% baseline vs 61% baseline, p = 0.038) but took fewer breaths (840 vs 1404 breaths, p = 0.017) than T-IMT participants. Inspiratory work was similar between groups (64,789 vs 65,910 (% PImax × number of breaths), p = 0.535).
Conclusions: Our findings support both methods of IMT as the change in PImax and inspiratory work were similar between groups. However, daily high-intensity F-IMT with intermittent supervision, required fewer breaths and less participant and therapist time. Future studies should examine optimal dosage and supervision required to achieve increased PImax.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


