{"title":"Central and peripheral pulmonary sclerosing pneumocytomas: multi-phase CT study and comparison with Ki-67.","authors":"Yanli Zhang, Chao Ran, Wei Li","doi":"10.2478/raon-2023-0042","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study aimed to evaluate the multi-phase CT findings of central and peripheral pulmonary sclerosing pneumocytomas (PSPs) and compared them with Ki-67 to reveal their neoplastic nature.</p><p><strong>Patients and methods: </strong>Multi-phase CT and clinical data of 33 PSPs (15 central PSPs and 18 peripheral PSPs) were retrospectively analyzed and compared their multi-phase CT features and Ki-67 levels.</p><p><strong>Results: </strong>For quantitative indicators, central PSPs were larger than peripheral PSPs (10.39 ± 3.25 cm<sup>3</sup> <i>vs.</i> 4.65 ± 2.61 cm<sup>3</sup>, P = 0.013), and tumor size was negatively correlated with acceleration index (r = -0.845, P < 0.001). The peak enhancement of central PSPs appeared in the delayed phase, with a longer time to peak enhancement (TTP, 100.81 ± 19.01 s), lower acceleration index (0.63 ± 0.17), progressive enhancement, and higher Ki-67 level. The peak enhancement of peripheral PSPs appeared in the venous phase, with the shorter TTP (62.67 ± 20.96 s, P < 0.001), higher acceleration index (0.99 ± 0.25, P < 0.001), enhancement washout, and lower Ki-67 level. For qualitative indicators, the overlying vessel sign (86.67% <i>vs.</i> 44.44%, P = 0.027), prominent pulmonary artery sign (73.33% <i>vs.</i> 27.78%, P = 0.015), and obstructive inflammation/atelectasis (26.67% <i>vs.</i> 0%, P = 0.033) were more common in central PSPs, while peripheral PSPs were more common with halo sign (38.89% <i>vs.</i> 6.67%, P = 0.046).</p><p><strong>Conclusions: </strong>The location of PSP is a possible contributing factor to its diverse imaging-pathological findings. The tumor size, multi-phase enhancement, qualitative signs, and Ki-67 were different between central and peripheral PSPs. Combined tumor size, multi-phase findings, and Ki-67 level are helpful to reveal the nature of the borderline tumor.</p>","PeriodicalId":21034,"journal":{"name":"Radiology and Oncology","volume":"57 3","pages":"310-316"},"PeriodicalIF":2.1000,"publicationDate":"2023-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10476905/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiology and Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2478/raon-2023-0042","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study aimed to evaluate the multi-phase CT findings of central and peripheral pulmonary sclerosing pneumocytomas (PSPs) and compared them with Ki-67 to reveal their neoplastic nature.
Patients and methods: Multi-phase CT and clinical data of 33 PSPs (15 central PSPs and 18 peripheral PSPs) were retrospectively analyzed and compared their multi-phase CT features and Ki-67 levels.
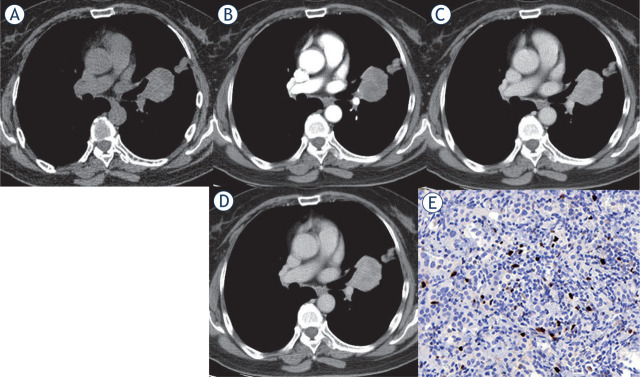
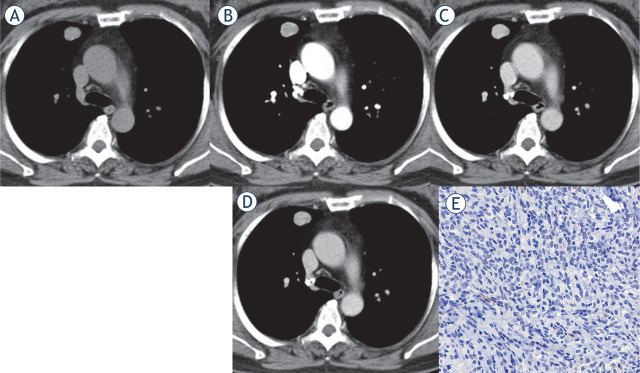
Results: For quantitative indicators, central PSPs were larger than peripheral PSPs (10.39 ± 3.25 cm3vs. 4.65 ± 2.61 cm3, P = 0.013), and tumor size was negatively correlated with acceleration index (r = -0.845, P < 0.001). The peak enhancement of central PSPs appeared in the delayed phase, with a longer time to peak enhancement (TTP, 100.81 ± 19.01 s), lower acceleration index (0.63 ± 0.17), progressive enhancement, and higher Ki-67 level. The peak enhancement of peripheral PSPs appeared in the venous phase, with the shorter TTP (62.67 ± 20.96 s, P < 0.001), higher acceleration index (0.99 ± 0.25, P < 0.001), enhancement washout, and lower Ki-67 level. For qualitative indicators, the overlying vessel sign (86.67% vs. 44.44%, P = 0.027), prominent pulmonary artery sign (73.33% vs. 27.78%, P = 0.015), and obstructive inflammation/atelectasis (26.67% vs. 0%, P = 0.033) were more common in central PSPs, while peripheral PSPs were more common with halo sign (38.89% vs. 6.67%, P = 0.046).
Conclusions: The location of PSP is a possible contributing factor to its diverse imaging-pathological findings. The tumor size, multi-phase enhancement, qualitative signs, and Ki-67 were different between central and peripheral PSPs. Combined tumor size, multi-phase findings, and Ki-67 level are helpful to reveal the nature of the borderline tumor.
背景:本研究旨在评价中枢性和外周性肺硬化性肺细胞瘤(PSPs)的多期CT表现,并与Ki-67进行比较,以揭示其肿瘤性质。患者及方法:回顾性分析33例PSPs(15例中枢性PSPs, 18例外周性PSPs)的多期CT及临床资料,比较其多期CT特征及Ki-67水平。结果:在定量指标上,中枢PSPs大于外周PSPs(10.39±3.25 cm3 vs. 4.65±2.61 cm3, P = 0.013),肿瘤大小与加速指数呈负相关(r = -0.845, P < 0.001)。中枢PSPs的峰值增强出现在延迟期,峰值增强时间较长(TTP为100.81±19.01 s),加速指数较低(0.63±0.17),逐渐增强,Ki-67水平较高。外周PSPs增强高峰出现在静脉期,TTP较短(62.67±20.96 s, P < 0.001),加速指数较高(0.99±0.25,P < 0.001),增强洗脱,Ki-67水平较低。定性指标方面,中枢性PSPs以覆盖血管征象(86.67% vs. 44.44%, P = 0.027)、肺动脉突出征象(73.33% vs. 27.78%, P = 0.015)、阻塞性炎症/肺不张(26.67% vs. 0%, P = 0.033)较多,外周性PSPs以晕征较多(38.89% vs. 6.67%, P = 0.046)。结论:PSP的位置可能是其不同影像病理表现的一个因素。中枢性和外周性PSPs的肿瘤大小、多期增强、定性征象和Ki-67均有差异。结合肿瘤大小、多期表现和Ki-67水平,有助于揭示交界性肿瘤的性质。
期刊介绍:
Radiology and Oncology is a multidisciplinary journal devoted to the publishing original and high quality scientific papers and review articles, pertinent to diagnostic and interventional radiology, computerized tomography, magnetic resonance, ultrasound, nuclear medicine, radiotherapy, clinical and experimental oncology, radiobiology, medical physics and radiation protection. Therefore, the scope of the journal is to cover beside radiology the diagnostic and therapeutic aspects in oncology, which distinguishes it from other journals in the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


