Ashraf M Abdel Aal, Islam Nouh, Mohamed Abdel Azeem, Ahmed M Al Adl, Basheer N Elmohamady
{"title":"Prediction of surgical decision and postoperative renal function using RENAL nephrometry score for localized renal masses: A prospective study.","authors":"Ashraf M Abdel Aal, Islam Nouh, Mohamed Abdel Azeem, Ahmed M Al Adl, Basheer N Elmohamady","doi":"10.4103/ua.ua_25_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The purpose of the study is to assess the value of RENAL nephrometry score (RNS) in predicting surgical decisions, complications, and decreases in kidney function in patients with localized renal tumors.</p><p><strong>Methods: </strong>Cases with solitary, solid, and enhancing renal masses were included, scheduled for nephron-sparing surgery (NSS), and assessed using routine laboratory and radiological data necessary for calculating the RENAL score. The primary endpoint was conversion to radical nephrectomy (RN), while the secondary endpoint was the prediction of a drop in renal function assessed by postoperative estimated glomerular filtration rate (eGFR) at the last follow-up visit compared with the preoperative values. The association between the scoring system and perioperative outcomes was evaluated.</p><p><strong>Results: </strong>In all, 84 cases were included, NSS was accomplished in 67 cases while conversion to RN was mandatory in 17 patients, median (interquartile range) RENAL score was 6.2 (4-10) for NSS and 9.7 (6-12) for RN (<i>P</i> < 0.001). Higher grades of complications were observed in the high-complexity subgroup. eGFR was 79.8 that dropped to 75.6 ml/min/1.73 m<sup>2</sup> in the late value in patients who underwent NSS, while it was 82.9 that dropped to 58.3 ml/min/1.73 m<sup>2</sup> in the late value in patients who converted into RN (<i>P</i> < 0.001). The percentage of drop in eGFR was significantly higher in the moderate and high-risk groups, which was positively correlated with the warm ischemia time. Regression analysis revealed that the continuous RENAL score was a more significant predictor of conversion to RN than tumor size alone. In the 67 NNS cases, the percentage decrease in eGFR was predicted using the continuous RENAL score.</p><p><strong>Conclusion: </strong>The RNS is a significant predictor of conversion to RN and can predict the percentage decrease in eGFR after NSS. Further investigations and follow-ups are necessary.</p>","PeriodicalId":23633,"journal":{"name":"Urology Annals","volume":"15 3","pages":"289-294"},"PeriodicalIF":0.8000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a6/99/UA-15-289.PMC10471816.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Urology Annals","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ua.ua_25_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/16 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The purpose of the study is to assess the value of RENAL nephrometry score (RNS) in predicting surgical decisions, complications, and decreases in kidney function in patients with localized renal tumors.
Methods: Cases with solitary, solid, and enhancing renal masses were included, scheduled for nephron-sparing surgery (NSS), and assessed using routine laboratory and radiological data necessary for calculating the RENAL score. The primary endpoint was conversion to radical nephrectomy (RN), while the secondary endpoint was the prediction of a drop in renal function assessed by postoperative estimated glomerular filtration rate (eGFR) at the last follow-up visit compared with the preoperative values. The association between the scoring system and perioperative outcomes was evaluated.
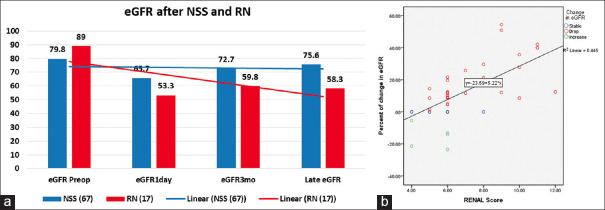
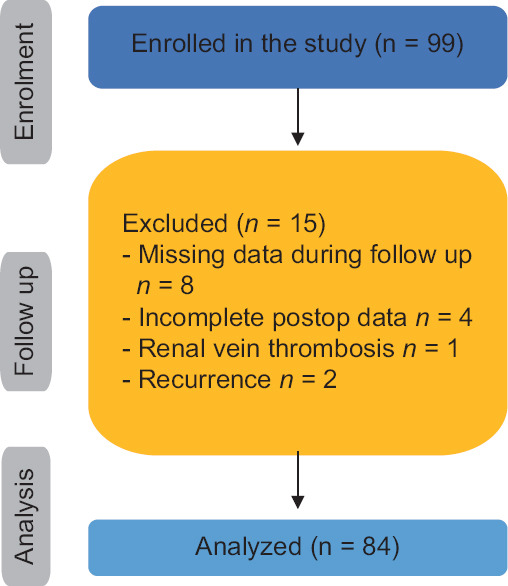
Results: In all, 84 cases were included, NSS was accomplished in 67 cases while conversion to RN was mandatory in 17 patients, median (interquartile range) RENAL score was 6.2 (4-10) for NSS and 9.7 (6-12) for RN (P < 0.001). Higher grades of complications were observed in the high-complexity subgroup. eGFR was 79.8 that dropped to 75.6 ml/min/1.73 m2 in the late value in patients who underwent NSS, while it was 82.9 that dropped to 58.3 ml/min/1.73 m2 in the late value in patients who converted into RN (P < 0.001). The percentage of drop in eGFR was significantly higher in the moderate and high-risk groups, which was positively correlated with the warm ischemia time. Regression analysis revealed that the continuous RENAL score was a more significant predictor of conversion to RN than tumor size alone. In the 67 NNS cases, the percentage decrease in eGFR was predicted using the continuous RENAL score.
Conclusion: The RNS is a significant predictor of conversion to RN and can predict the percentage decrease in eGFR after NSS. Further investigations and follow-ups are necessary.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


