Therapeutic outcomes of early and delayed endoscopic retrograde cholangiopancreatography and percutaneous transhepatic cholangial drainage in patients with obstructive severe acute biliary pancreatitis.
Xue Ling Zhang, Jia Huan Sun, Yue Wu, Min Xie, Cong Cong Li, Dong Lv, Wei Yu, Pei Lin Cui
{"title":"Therapeutic outcomes of early and delayed endoscopic retrograde cholangiopancreatography and percutaneous transhepatic cholangial drainage in patients with obstructive severe acute biliary pancreatitis.","authors":"Xue Ling Zhang, Jia Huan Sun, Yue Wu, Min Xie, Cong Cong Li, Dong Lv, Wei Yu, Pei Lin Cui","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Obstructive severe acute biliary pancreatitis (SABP) is a clinical emergency with a high rate of mortality that can be alleviated by endoscopic retrograde cholangiopancreatography (ERCP) and percutaneous transhepatic cholangial drainage (PTCD) selectively. However, the optimal timing of ERCP and PTCD requires elucidation.</p><p><strong>Aim: </strong>The aim of this study was to evaluate outcome parameters in patients with SABP subjected to ERCP and PTCD compared to SABP patients who were not subjected to any form of invasive intervention.</p><p><strong>Methods: </strong>A total of 62 patients with obstructive SABP who had been treated from July 2013 to July 2019 were included in this retrospective case-control study and stratified into a PTCD group (N = 22), ERCP group (N = 24), and conservative treatment group (N = 16, control). Patients in the PTCD and ERCP groups were substratified into early (≤72 h) and delayed (>72 h) treatment groups based on the timing of the intervention after diagnosis. Clinical chemistry, hospitalization days, liver function, abdominal pain, and complications were determined to assess the treatment efficacy and safety of each modality and to establish the optimal timing for PTCD and ERCP.</p><p><strong>Results: </strong>The average hospitalization time, time to abdominal pain relief, and time to normalization of hematological and clinical chemistry parameters (leukocyte count, amylase, alanine transaminase [ALT], and total bilirubin [TBiL]) were shorter in the PTCD and ERCP groups compared to the conservative treatment group (<i>p</i> < 0.05). The average hospitalization time in the ERCP group (16.7 ± 4.0 d) was shorter compared to the PTCD group (19.6 ± 4.3 d) (<i>p</i> < 0.05). Compared to the conservative treatment group (62.5%), there were more complications in patients treated with ERCP and PTCD (<i>p</i> < 0.05). In the early ERCP group, the average hospitalization time (13.9 ± 3.3 d) and the time to normalization of leukocyte count (6.3 ± 0.9 d) and TBiL (9.1 ± 2.0 d) were lower than in the delayed ERCP group (18.6 ± 4.1 d, 9.9 ± 2.4 d, 11.8 ± 2.9 d, respectively) and early PTCD group (16.4 ± 3.7 d, 8.5 ± 2.1 d, 10.9 ± 3.1 d, respectively) (<i>p</i> < 0.05). In the delayed ERCP group, the average hospitalization time (18.6 ± 4.1 d) and ALT recovery time (12.2 ± 2.6 d) were lower than in the delayed PTCD group (21.9 ± 4.3 d and 14.9 ± 3.9 d, respectively) (<i>p</i> < 0.05).</p><p><strong>Conclusions: </strong>ERCP and PTCD effectively relieve SABP-associated biliary obstruction with comparable overall incidence of complications. It is recommended that ERCP is performed within 72 h after diagnosis; and PTCD drainage may be considered an alternative approach in cases where patients are unable or unwilling to undergo ERCP, or when ERCP is unsuccessful.</p><p><strong>Relevance for patients: </strong>ERCP and PTCD in patients with obstructive SABP can resolve biliary obstruction and delay progression of the disease. Performing ERCP and PTCD within 72 h (i.e., optimal treatment time window) can be beneficial to patients, especially in terms of post-operative recovery. Visual biliary endoscopy (oral or percutaneous transhepatic) may be used for concomitant therapeutic interventions in the biliary system.</p>","PeriodicalId":15482,"journal":{"name":"Journal of Clinical and Translational Research","volume":"9 3","pages":"160-167"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/60/f1/jclintranslres-2023-9-3-160.PMC10339408.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Translational Research","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Obstructive severe acute biliary pancreatitis (SABP) is a clinical emergency with a high rate of mortality that can be alleviated by endoscopic retrograde cholangiopancreatography (ERCP) and percutaneous transhepatic cholangial drainage (PTCD) selectively. However, the optimal timing of ERCP and PTCD requires elucidation.
Aim: The aim of this study was to evaluate outcome parameters in patients with SABP subjected to ERCP and PTCD compared to SABP patients who were not subjected to any form of invasive intervention.
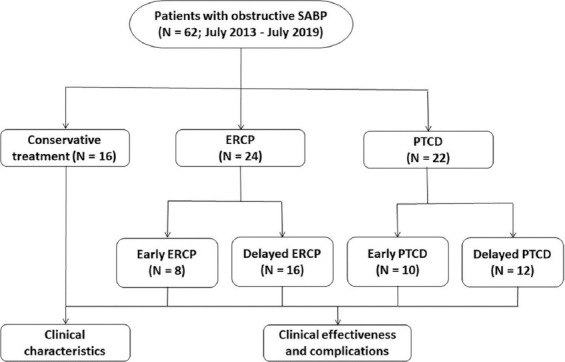
Methods: A total of 62 patients with obstructive SABP who had been treated from July 2013 to July 2019 were included in this retrospective case-control study and stratified into a PTCD group (N = 22), ERCP group (N = 24), and conservative treatment group (N = 16, control). Patients in the PTCD and ERCP groups were substratified into early (≤72 h) and delayed (>72 h) treatment groups based on the timing of the intervention after diagnosis. Clinical chemistry, hospitalization days, liver function, abdominal pain, and complications were determined to assess the treatment efficacy and safety of each modality and to establish the optimal timing for PTCD and ERCP.
Results: The average hospitalization time, time to abdominal pain relief, and time to normalization of hematological and clinical chemistry parameters (leukocyte count, amylase, alanine transaminase [ALT], and total bilirubin [TBiL]) were shorter in the PTCD and ERCP groups compared to the conservative treatment group (p < 0.05). The average hospitalization time in the ERCP group (16.7 ± 4.0 d) was shorter compared to the PTCD group (19.6 ± 4.3 d) (p < 0.05). Compared to the conservative treatment group (62.5%), there were more complications in patients treated with ERCP and PTCD (p < 0.05). In the early ERCP group, the average hospitalization time (13.9 ± 3.3 d) and the time to normalization of leukocyte count (6.3 ± 0.9 d) and TBiL (9.1 ± 2.0 d) were lower than in the delayed ERCP group (18.6 ± 4.1 d, 9.9 ± 2.4 d, 11.8 ± 2.9 d, respectively) and early PTCD group (16.4 ± 3.7 d, 8.5 ± 2.1 d, 10.9 ± 3.1 d, respectively) (p < 0.05). In the delayed ERCP group, the average hospitalization time (18.6 ± 4.1 d) and ALT recovery time (12.2 ± 2.6 d) were lower than in the delayed PTCD group (21.9 ± 4.3 d and 14.9 ± 3.9 d, respectively) (p < 0.05).
Conclusions: ERCP and PTCD effectively relieve SABP-associated biliary obstruction with comparable overall incidence of complications. It is recommended that ERCP is performed within 72 h after diagnosis; and PTCD drainage may be considered an alternative approach in cases where patients are unable or unwilling to undergo ERCP, or when ERCP is unsuccessful.
Relevance for patients: ERCP and PTCD in patients with obstructive SABP can resolve biliary obstruction and delay progression of the disease. Performing ERCP and PTCD within 72 h (i.e., optimal treatment time window) can be beneficial to patients, especially in terms of post-operative recovery. Visual biliary endoscopy (oral or percutaneous transhepatic) may be used for concomitant therapeutic interventions in the biliary system.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


