Impact of conversion at time of minimally invasive pancreaticoduodenectomy on perioperative and long-term outcomes: Review of the National Cancer Database.
Jennifer Palacio, Daisy Sanchez, Shenae Samuels, Bar Y Ainuz, Raelynn M Vigue, Waleem E Hernandez, Christopher J Gannon, Omar H Llaguna
{"title":"Impact of conversion at time of minimally invasive pancreaticoduodenectomy on perioperative and long-term outcomes: Review of the National Cancer Database.","authors":"Jennifer Palacio, Daisy Sanchez, Shenae Samuels, Bar Y Ainuz, Raelynn M Vigue, Waleem E Hernandez, Christopher J Gannon, Omar H Llaguna","doi":"10.14701/ahbps.22-101","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>Current literature presents limited data regarding outcomes following conversion at the time of minimally invasive pancreaticoduodenectomy (MI-PD).</p><p><strong>Methods: </strong>The National Cancer Database was queried for patients who underwent pancreaticoduodenectomy. Patients were stratified into three groups: MI-PD, converted to open pancreaticoduodenectomy (CO-PD), and open pancreaticoduodenectomy (O-PD). Multivariable modeling was applied to compare outcomes of MI-PD and CO-PD to those of O-PD.</p><p><strong>Results: </strong>Of 17,570 patients identified, 12.5%, 4.2%, and 83.4% underwent MI-PD, CO-PD, and O-PD, respectively. Robotic pancreaticoduodenectomy (R-PD) resulted in a higher lymph node yield (n = 23.2 ± 12.2) even when requiring conversion (n = 22.4 ± 13.2, <i>p</i> < 0.001). Margin positivity was higher in the CO-PD group (26.6%) than in the MI-PD group (21.3%) and the O-PD (22.6%) group (<i>p</i> = 0.017). Length of stay was shorter in the MI-PD group (laparoscopic pancreaticoduodenectomy 10.4 ± 8.6, R-PD 10.6 ± 8.8) and the robotic converted to open group (10.7 ± 6.4) than in the laparoscopic converted to open group (11.2 ± 9) and the O-PD group (11.5 ± 8.9) (<i>p</i> < 0.001). After adjusting for patient and tumor characteristics, both MI-PD (odds ratio = 1.40; <i>p</i> < 0.001) and CO-PD (odds ratio = 1.24; <i>p</i> = 0.020) were significantly associated with an increased likelihood of long-term survival.</p><p><strong>Conclusions: </strong>CO-PD does not negatively impact perioperative or oncologic outcomes.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":"27 3","pages":"292-300"},"PeriodicalIF":1.1000,"publicationDate":"2023-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ef/d4/ahbps-27-3-292.PMC10472115.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.22-101","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Backgrounds/aims: Current literature presents limited data regarding outcomes following conversion at the time of minimally invasive pancreaticoduodenectomy (MI-PD).
Methods: The National Cancer Database was queried for patients who underwent pancreaticoduodenectomy. Patients were stratified into three groups: MI-PD, converted to open pancreaticoduodenectomy (CO-PD), and open pancreaticoduodenectomy (O-PD). Multivariable modeling was applied to compare outcomes of MI-PD and CO-PD to those of O-PD.
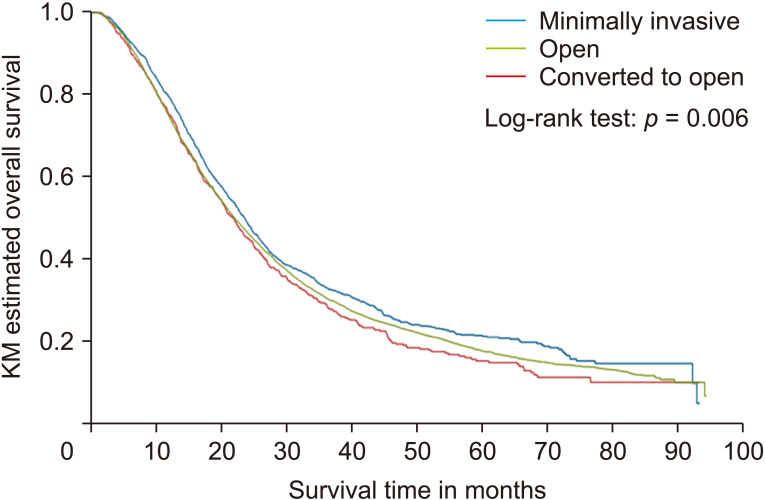
Results: Of 17,570 patients identified, 12.5%, 4.2%, and 83.4% underwent MI-PD, CO-PD, and O-PD, respectively. Robotic pancreaticoduodenectomy (R-PD) resulted in a higher lymph node yield (n = 23.2 ± 12.2) even when requiring conversion (n = 22.4 ± 13.2, p < 0.001). Margin positivity was higher in the CO-PD group (26.6%) than in the MI-PD group (21.3%) and the O-PD (22.6%) group (p = 0.017). Length of stay was shorter in the MI-PD group (laparoscopic pancreaticoduodenectomy 10.4 ± 8.6, R-PD 10.6 ± 8.8) and the robotic converted to open group (10.7 ± 6.4) than in the laparoscopic converted to open group (11.2 ± 9) and the O-PD group (11.5 ± 8.9) (p < 0.001). After adjusting for patient and tumor characteristics, both MI-PD (odds ratio = 1.40; p < 0.001) and CO-PD (odds ratio = 1.24; p = 0.020) were significantly associated with an increased likelihood of long-term survival.
Conclusions: CO-PD does not negatively impact perioperative or oncologic outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


