Ahmed M Harraz, Adel Nabeeh, Ramy Elbaz, Abdalla Abdelhamid, Mohamed Tharwat, Amr A Elbakry, Ahmed S El-Hefnawy, Ahmed El-Assmy, Ahmed Mosbah, Mohamed H Zahran
{"title":"Could the bulbar urethral end location on the cystourethrogram predict the outcome after posterior urethroplasty for pelvic fracture urethral injury?","authors":"Ahmed M Harraz, Adel Nabeeh, Ramy Elbaz, Abdalla Abdelhamid, Mohamed Tharwat, Amr A Elbakry, Ahmed S El-Hefnawy, Ahmed El-Assmy, Ahmed Mosbah, Mohamed H Zahran","doi":"10.1080/2090598X.2022.2138119","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To identify cystourethrogram (CUG) findings that independently predict the outcome of posterior urethroplasty (PU) following pelvic fracture urethral injury (PFUI).</p><p><strong>Methods: </strong>Findings of CUG included the location of the proximal end of the bulbar urethra in zones A (superficial) or B (deep) according to its relationship with the pubic arch. Others included the presence of pelvic arch fracture, bladder neck, and posterior urethral appearance. The primary outcome was the need for reintervention either endoscopically or by redo urethroplasty. Independent predictors were modeled using a logistic regression model and a nomogram was constructed and internally validated using 100-bootstrap resampling. Time-to-event analysis was performed to validate the results.</p><p><strong>Results: </strong>A total of 196 procedures in 158 patients were analyzed. The success rate was 83.7% with 32 (16.3%) procedures requiring direct vision internal urethrotomy, urethroplasty, or both in 13 (6.6%), 12 (6.1%), and 7 (3.6%) patients, respectively. On multivariate analysis, bulbar urethral end located at zone B (odds ratio [OR]: 3.1; 95% confidence interval [CI]: 1.1-8.5; p = 0.02), pubic arch fracture (OR: 3.9; 95%CI: 1.5-9.7; p = 0.003), and previous urethroplasty (OR: 4.2; 95% CI: 1.8-10.1; p = 0.001) were independent predictors. The same predictors were significant in the time-to-event analysis. The nomogram discrimination was 77.3% and 75% in the current data and after validation.</p><p><strong>Conclusions: </strong>The location of the proximal end of the bulbar urethra and redo urethroplasty could predict the need for reintervention after PU for PFUI. The nomogram could be used preoperatively for patient counseling and procedure planning.</p>","PeriodicalId":8113,"journal":{"name":"Arab Journal of Urology","volume":"21 2","pages":"94-101"},"PeriodicalIF":1.2000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10208150/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arab Journal of Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/2090598X.2022.2138119","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To identify cystourethrogram (CUG) findings that independently predict the outcome of posterior urethroplasty (PU) following pelvic fracture urethral injury (PFUI).
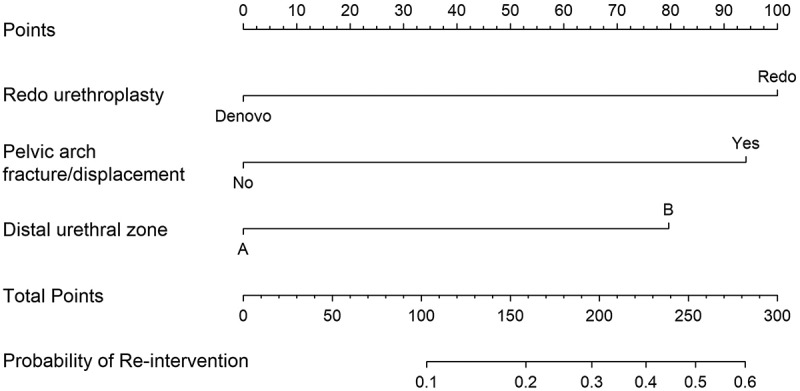
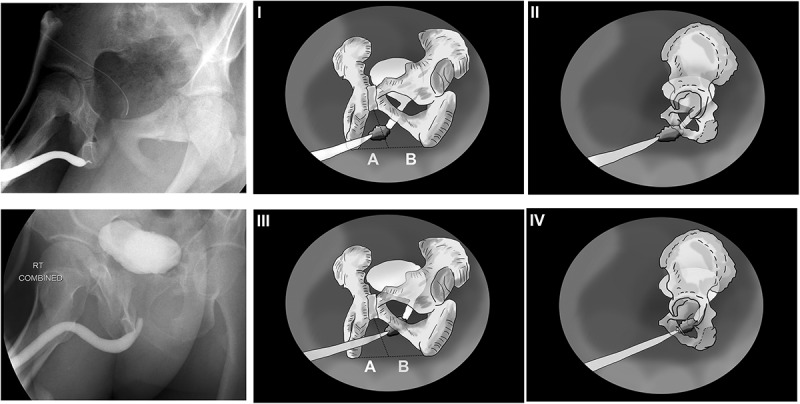
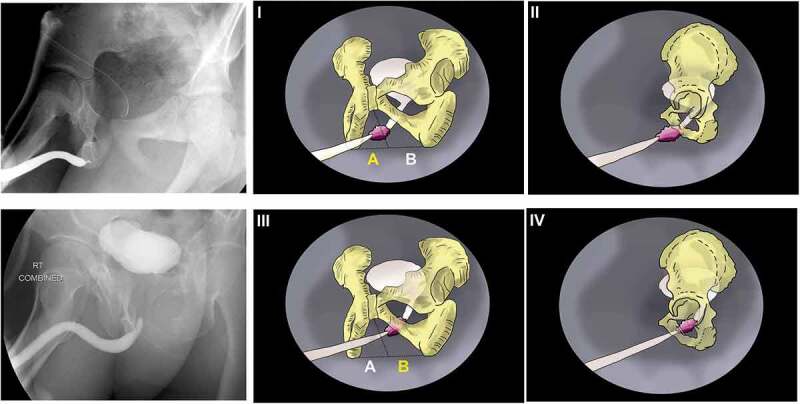
Methods: Findings of CUG included the location of the proximal end of the bulbar urethra in zones A (superficial) or B (deep) according to its relationship with the pubic arch. Others included the presence of pelvic arch fracture, bladder neck, and posterior urethral appearance. The primary outcome was the need for reintervention either endoscopically or by redo urethroplasty. Independent predictors were modeled using a logistic regression model and a nomogram was constructed and internally validated using 100-bootstrap resampling. Time-to-event analysis was performed to validate the results.
Results: A total of 196 procedures in 158 patients were analyzed. The success rate was 83.7% with 32 (16.3%) procedures requiring direct vision internal urethrotomy, urethroplasty, or both in 13 (6.6%), 12 (6.1%), and 7 (3.6%) patients, respectively. On multivariate analysis, bulbar urethral end located at zone B (odds ratio [OR]: 3.1; 95% confidence interval [CI]: 1.1-8.5; p = 0.02), pubic arch fracture (OR: 3.9; 95%CI: 1.5-9.7; p = 0.003), and previous urethroplasty (OR: 4.2; 95% CI: 1.8-10.1; p = 0.001) were independent predictors. The same predictors were significant in the time-to-event analysis. The nomogram discrimination was 77.3% and 75% in the current data and after validation.
Conclusions: The location of the proximal end of the bulbar urethra and redo urethroplasty could predict the need for reintervention after PU for PFUI. The nomogram could be used preoperatively for patient counseling and procedure planning.
期刊介绍:
The Arab Journal of Urology is a peer-reviewed journal that strives to provide a high standard of research and clinical material to the widest possible urological community worldwide. The journal encompasses all aspects of urology including: urological oncology, urological reconstructive surgery, urodynamics, female urology, pediatric urology, endourology, transplantation, erectile dysfunction, and urinary infections and inflammations. The journal provides reviews, original articles, editorials, surgical techniques, cases reports and correspondence. Urologists, oncologists, pathologists, radiologists and scientists are invited to submit their contributions to make the Arab Journal of Urology a viable international forum for the practical, timely and state-of-the-art clinical urology and basic urological research.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


