Abdullah Alkhayal, Sahar Aljumaiah, Abdullah Alhagbani, Muhannad Alnahdi, Saad Abumelha, Khalid Alrabeeah
{"title":"Varicocelectomy for scrotal pain: Is it effective?","authors":"Abdullah Alkhayal, Sahar Aljumaiah, Abdullah Alhagbani, Muhannad Alnahdi, Saad Abumelha, Khalid Alrabeeah","doi":"10.4103/UA.UA_64_20","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Varicocelectomy is the prevailing management of scrotal pain secondary to varicocele. However, the literature is controversial on this topic. Some data showed that pain may persist after the surgery even if the varicocele is not detected postoperatively.</p><p><strong>Objectives: </strong>The objectives of the study were to identify the effect of varicocelectomy in patients with chronic scrotal pain, to report the association between the clinical grade and postoperative pain resolution, and to identify the need for a secondary procedure after varicocelectomy to control the pain.</p><p><strong>Materials and methods: </strong>This was a retrospective study of 47 patients who underwent varicocelectomy between March 2016 and December 2018.</p><p><strong>Results: </strong>Postoperatively, the pain totally resolved after surgery in 64.3% of patients with scrotal pain; it improved in 21.4%, 11.9% have persistent pain, and the pain got worse in only 2.4%. Our study showed 100% complete resolution or improvement with Grade I, 85.7% in Grade II, and 81.3% in Grade III. In addition, all patients who underwent bilateral varicocelectomy had pain that either completely resolved or improved postoperatively. On the other hand, all patients who had persistent pain or pain worsening postoperatively had unilateral varicocelectomy. An additional intervention for postoperative pain control was needed in only 14% of patients, 7% of them underwent embolization, 4.7% had a cord block, and 2.3% were sent to a pain clinic.</p><p><strong>Conclusion: </strong>Varicocelectomy offers good outcomes in most patients with varicocele-related scrotal pain. The most significant predictor for success was low grade and bilaterality. However, there is a subset of patients whose symptoms will not improve postoperatively. Careful preoperative counseling and expectation management are crucial when discussing surgical options for those patients.</p>","PeriodicalId":23633,"journal":{"name":"Urology Annals","volume":"15 3","pages":"311-314"},"PeriodicalIF":0.8000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dc/e6/UA-15-311.PMC10471819.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Urology Annals","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/UA.UA_64_20","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/17 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Varicocelectomy is the prevailing management of scrotal pain secondary to varicocele. However, the literature is controversial on this topic. Some data showed that pain may persist after the surgery even if the varicocele is not detected postoperatively.
Objectives: The objectives of the study were to identify the effect of varicocelectomy in patients with chronic scrotal pain, to report the association between the clinical grade and postoperative pain resolution, and to identify the need for a secondary procedure after varicocelectomy to control the pain.
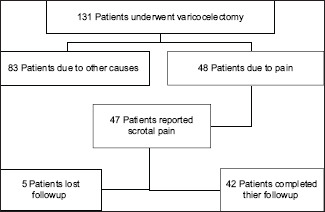
Materials and methods: This was a retrospective study of 47 patients who underwent varicocelectomy between March 2016 and December 2018.
Results: Postoperatively, the pain totally resolved after surgery in 64.3% of patients with scrotal pain; it improved in 21.4%, 11.9% have persistent pain, and the pain got worse in only 2.4%. Our study showed 100% complete resolution or improvement with Grade I, 85.7% in Grade II, and 81.3% in Grade III. In addition, all patients who underwent bilateral varicocelectomy had pain that either completely resolved or improved postoperatively. On the other hand, all patients who had persistent pain or pain worsening postoperatively had unilateral varicocelectomy. An additional intervention for postoperative pain control was needed in only 14% of patients, 7% of them underwent embolization, 4.7% had a cord block, and 2.3% were sent to a pain clinic.
Conclusion: Varicocelectomy offers good outcomes in most patients with varicocele-related scrotal pain. The most significant predictor for success was low grade and bilaterality. However, there is a subset of patients whose symptoms will not improve postoperatively. Careful preoperative counseling and expectation management are crucial when discussing surgical options for those patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


