Jorge A Barrero, Laura M Villamil-Camargo, Jose N Imaz, Karen Arciniegas-Villa, Jorge A Rubio-Romero
{"title":"Maternal Serum Activin A, Inhibin A and Follistatin-Related Proteins across Preeclampsia: Insights into Their Role in Pathogenesis and Prediction.","authors":"Jorge A Barrero, Laura M Villamil-Camargo, Jose N Imaz, Karen Arciniegas-Villa, Jorge A Rubio-Romero","doi":"10.34763/jmotherandchild.20232701.d-23-00002","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Within the endocrine-paracrine signalling network at the maternal-foetal interface, the activin-inhibin-follistatin system modulates extravillous trophoblast invasion, suggesting a potential role in preeclampsia pathogenesis. This study aimed to compile the evidence published in the last decade regarding the variation in maternal serum activins, inhibin- and follistatin-related proteins in preeclamptic pregnancies compared to healthy pregnancies, and to discuss their role in predicting and understanding the pathophysiology of preeclampsia.</p><p><strong>Material and methods: </strong>A scoping review was conducted in MEDLINE, EMBASE and LILACS databases to identify studies published within the last ten years (2012-2022).</p><p><strong>Results: </strong>Thirty studies were included. None of the studies addressed maternal serum changes of isoforms different from activin A, inhibin A, follistatin, and follistatin-like 3. Sixteen studies evaluated the potential of these isoforms in predicting preeclampsia through the area under the curve from a receiver operating characteristic curve.</p><p><strong>Conclusions: </strong>In preeclampsia, inhibin A is upregulated in all trimesters, whereas activin A increases exclusively in the late second and third trimesters. Serum follistatin levels are reduced in women with preeclampsia during the late second and third trimesters. However, changes in follistatin-like 3 remain inconclusive. Inhibin A and activin A can potentially serve as biomarkers of early-onset preeclampsia based on the outcomes of the receiver operating characteristic curve analysis. Further investigations are encouraged to explore the feasibility of quantifying maternal serum levels of activin A and inhibin A as a clinical tool in early preeclampsia prediction.</p>","PeriodicalId":73842,"journal":{"name":"Journal of mother and child","volume":"27 1","pages":"119-133"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10438925/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of mother and child","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34763/jmotherandchild.20232701.d-23-00002","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
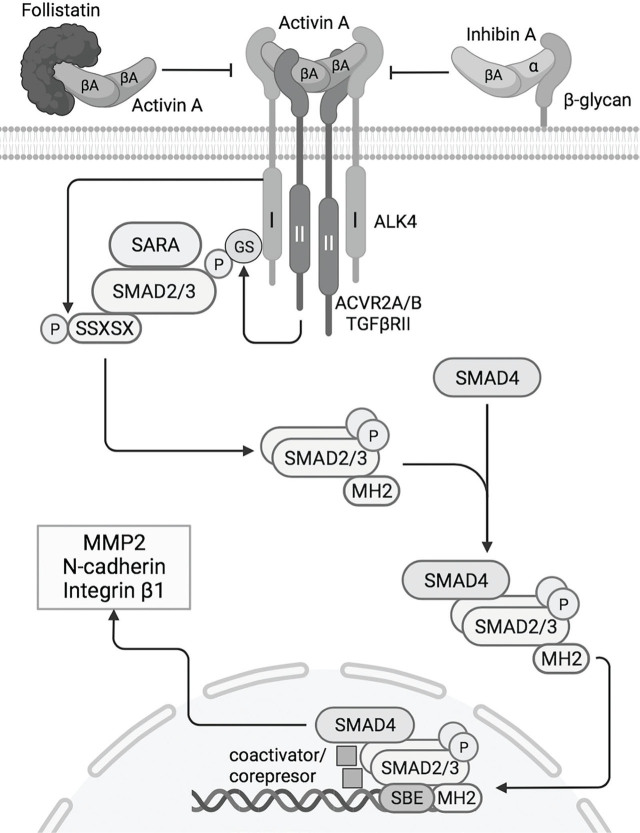
Background: Within the endocrine-paracrine signalling network at the maternal-foetal interface, the activin-inhibin-follistatin system modulates extravillous trophoblast invasion, suggesting a potential role in preeclampsia pathogenesis. This study aimed to compile the evidence published in the last decade regarding the variation in maternal serum activins, inhibin- and follistatin-related proteins in preeclamptic pregnancies compared to healthy pregnancies, and to discuss their role in predicting and understanding the pathophysiology of preeclampsia.
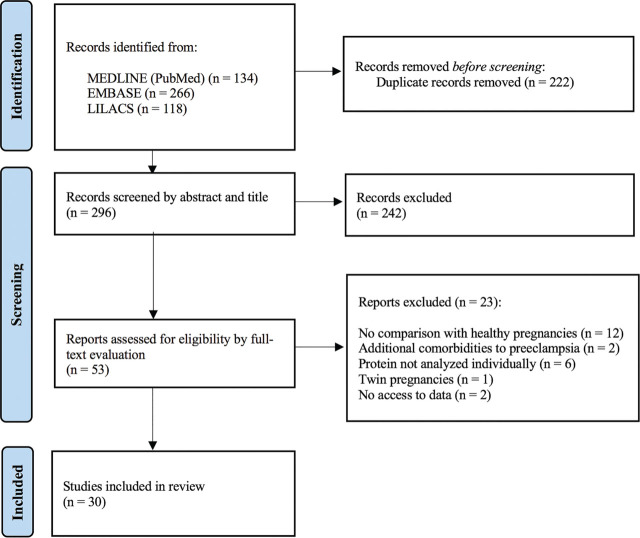
Material and methods: A scoping review was conducted in MEDLINE, EMBASE and LILACS databases to identify studies published within the last ten years (2012-2022).
Results: Thirty studies were included. None of the studies addressed maternal serum changes of isoforms different from activin A, inhibin A, follistatin, and follistatin-like 3. Sixteen studies evaluated the potential of these isoforms in predicting preeclampsia through the area under the curve from a receiver operating characteristic curve.
Conclusions: In preeclampsia, inhibin A is upregulated in all trimesters, whereas activin A increases exclusively in the late second and third trimesters. Serum follistatin levels are reduced in women with preeclampsia during the late second and third trimesters. However, changes in follistatin-like 3 remain inconclusive. Inhibin A and activin A can potentially serve as biomarkers of early-onset preeclampsia based on the outcomes of the receiver operating characteristic curve analysis. Further investigations are encouraged to explore the feasibility of quantifying maternal serum levels of activin A and inhibin A as a clinical tool in early preeclampsia prediction.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


