Greg A J Robertson, Amit Sinha, Thomas Hodkinson, Togay Koç
{"title":"Return to sport following toe phalanx fractures: A systematic review.","authors":"Greg A J Robertson, Amit Sinha, Thomas Hodkinson, Togay Koç","doi":"10.5312/wjo.v14.i6.471","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Evidence-based guidance on return to sport following toe phalanx fractures is limited.</p><p><strong>Aim: </strong>To systemically review all studies recording return to sport following toe phalanx fractures (both acute fractures and stress fractures), and to collate information on return rates to sport (RRS) and mean return times (RTS) to the sport.</p><p><strong>Methods: </strong>A systematic search of PubMed, MEDLINE, EMBASE, CINAHL, Cochrane Library, Physiotherapy Evidence Database, and Google Scholar was performed in December 2022 using the keywords 'Toe', 'Phalanx', 'Fracture', 'injury', 'athletes', 'sports', 'non-operative', 'conservative', 'operative', 'return to sport'. All studies which recorded RRS and RTS following toe phalanx fractures were included.</p><p><strong>Results: </strong>Thirteen studies were included: one retrospective cohort study and twelve case series. Seven studies reported on acute fractures. Six studies reported on stress fractures. For the acute fractures (<i>n</i> = 156), 63 were treated with primary conservative management (PCM), 6 with primary surgical management (PSM) (all displaced intra-articular (physeal) fractures of the great toe base of the proximal phalanx), 1 with secondary surgical management (SSM) and 87 did not specify treatment modality. For the stress fractures (<i>n</i> = 26), 23 were treated with PCM, 3 with PSM, and 6 with SSM. For acute fractures, RRS with PCM ranged from 0 to 100%, and RTS with PCM ranged from 1.2 to 24 wk. For acute fractures, RRS with PSM were all 100%, and RTS with PSM ranged from 12 to 24 wk. One case of an undisplaced intra-articular (physeal) fracture treated conservatively required conversion to SSM on refracture with a return to sport. For stress fractures, RRS with PCM ranged from 0% to 100%, and RTS with PCM ranged from 5 to 10 wk. For stress fractures, RRS with PSM were all 100%, and RTS with surgical management ranged from 10 to 16 wk. Six cases of conservatively-managed stress fractures required conversion to SSM. Two of these cases were associated with a prolonged delay to diagnosis (1 year, 2 years) and four cases with an underlying deformity [hallux valgus (<i>n</i> = 3), claw toe (<i>n</i> = 1)]. All six cases returned to the sport after SSM.</p><p><strong>Conclusion: </strong>The majority of sport-related toe phalanx fractures (acute and stress) are managed conservatively with overall satisfactory RRS and RTS. For acute fractures, surgical management is indicated for displaced, intra-articular (physeal) fractures, which offers satisfactory RRS and RTS. For stress fractures, surgical management is indicated for cases with delayed diagnosis and established non-union at presentation, or with significant underlying deformity: both can expect satisfactory RRS and RTS.</p>","PeriodicalId":47843,"journal":{"name":"World Journal of Orthopedics","volume":"14 6","pages":"471-484"},"PeriodicalIF":2.0000,"publicationDate":"2023-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4a/cd/WJO-14-471.PMC10292062.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5312/wjo.v14.i6.471","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Evidence-based guidance on return to sport following toe phalanx fractures is limited.
Aim: To systemically review all studies recording return to sport following toe phalanx fractures (both acute fractures and stress fractures), and to collate information on return rates to sport (RRS) and mean return times (RTS) to the sport.
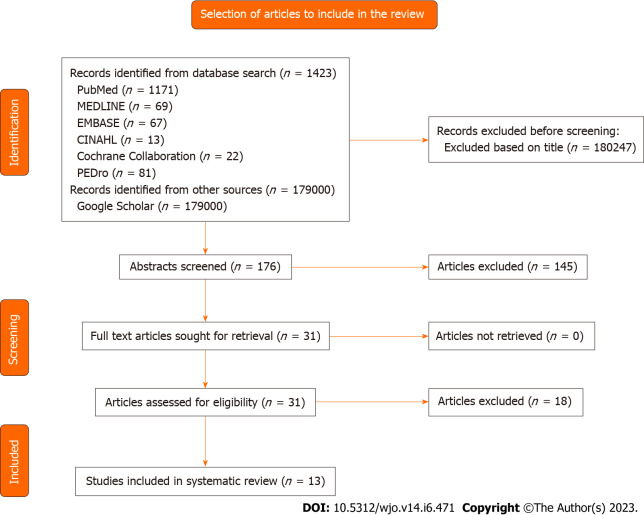
Methods: A systematic search of PubMed, MEDLINE, EMBASE, CINAHL, Cochrane Library, Physiotherapy Evidence Database, and Google Scholar was performed in December 2022 using the keywords 'Toe', 'Phalanx', 'Fracture', 'injury', 'athletes', 'sports', 'non-operative', 'conservative', 'operative', 'return to sport'. All studies which recorded RRS and RTS following toe phalanx fractures were included.
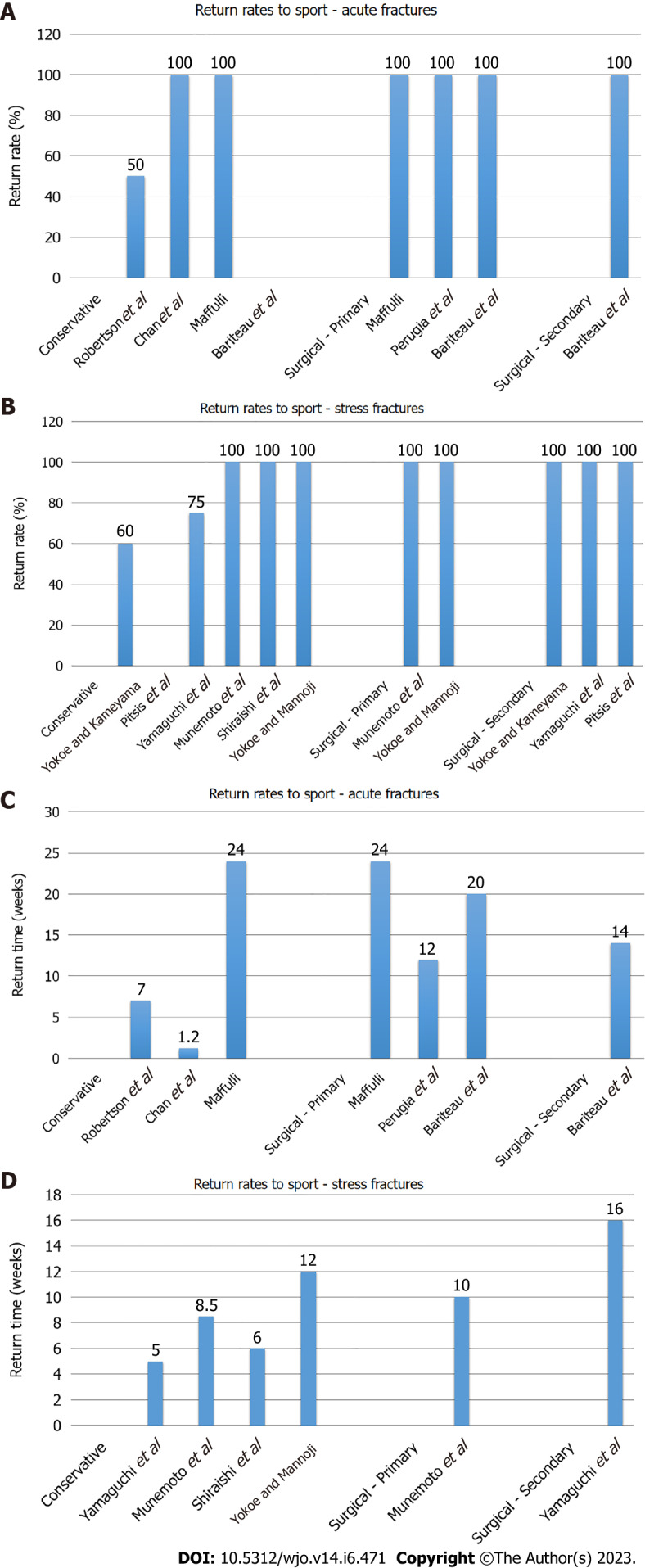
Results: Thirteen studies were included: one retrospective cohort study and twelve case series. Seven studies reported on acute fractures. Six studies reported on stress fractures. For the acute fractures (n = 156), 63 were treated with primary conservative management (PCM), 6 with primary surgical management (PSM) (all displaced intra-articular (physeal) fractures of the great toe base of the proximal phalanx), 1 with secondary surgical management (SSM) and 87 did not specify treatment modality. For the stress fractures (n = 26), 23 were treated with PCM, 3 with PSM, and 6 with SSM. For acute fractures, RRS with PCM ranged from 0 to 100%, and RTS with PCM ranged from 1.2 to 24 wk. For acute fractures, RRS with PSM were all 100%, and RTS with PSM ranged from 12 to 24 wk. One case of an undisplaced intra-articular (physeal) fracture treated conservatively required conversion to SSM on refracture with a return to sport. For stress fractures, RRS with PCM ranged from 0% to 100%, and RTS with PCM ranged from 5 to 10 wk. For stress fractures, RRS with PSM were all 100%, and RTS with surgical management ranged from 10 to 16 wk. Six cases of conservatively-managed stress fractures required conversion to SSM. Two of these cases were associated with a prolonged delay to diagnosis (1 year, 2 years) and four cases with an underlying deformity [hallux valgus (n = 3), claw toe (n = 1)]. All six cases returned to the sport after SSM.
Conclusion: The majority of sport-related toe phalanx fractures (acute and stress) are managed conservatively with overall satisfactory RRS and RTS. For acute fractures, surgical management is indicated for displaced, intra-articular (physeal) fractures, which offers satisfactory RRS and RTS. For stress fractures, surgical management is indicated for cases with delayed diagnosis and established non-union at presentation, or with significant underlying deformity: both can expect satisfactory RRS and RTS.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


