Kristina Ma, Emelie Carlestål, Anders Franco-Cereceda, Christian Olsson
{"title":"Reoperation or Aortic Regurgitation Progression after Reimplantation of the Aortic Valve (David's Procedure) Using the Valsalva Graft.","authors":"Kristina Ma, Emelie Carlestål, Anders Franco-Cereceda, Christian Olsson","doi":"10.1055/s-0043-1768968","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong> This study aimed to assess predictors of a composite endpoint (reoperation for aortic valve [AV] failure or aortic regurgitation [AR] grade ≥ 2) after reimplantation of the aortic valve (RAV) using the Valsalva graft.</p><p><strong>Methods: </strong> From 2012 to 2021, 112 patients underwent RAV in a single center. Clinical and echocardiographic data were collected retrospectively. Cox regression analysis was used to identify predictors of the composite endpoint. Kaplan-Meier methods were used for time-to-event analysis.</p><p><strong>Results: </strong> Median (interquartile range) age was 52 years (44, 62). Nineteen patients (17%) were operated for acute Type A aortic dissection, and the remainder for aortic root aneurysm, 60 mm or larger in 12/112 (11%). Thirty-day mortality was 1/112 (1%). During follow-up, four patients (3.6%) were reoperated for AV failure, and another nine patients (8.1%) developed AR grade ≥ 2. Overall estimated freedom from reoperation or AR grade ≥ 2 was 87% (95% confidence interval: 76-93%) at 5 years. Significantly lower estimated 5-year freedom from the composite endpoint was found in cases with simultaneous aortic valve repair (AVr; 77 vs. 90%, <i>p</i> = 0.007) and nearly significant for large (≥ 6 cm) aortic root diameter (82 vs. 87%, <i>p</i> = 0.055). In Cox's analysis, aortic root diameter and simultaneous AVr were independent predictors for the composite endpoint.</p><p><strong>Conclusion: </strong> Outcomes (survival, reoperation, freedom from AR grade ≥ 2) with RAV were good up to 11-year follow-up. Larger aortic root diameter and simultaneous AVr were identified as predictors for reoperation or AR grade ≥ 2. Long-term follow-up remains necessary to confirm adequate AV function.</p>","PeriodicalId":52392,"journal":{"name":"AORTA","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bb/18/10-1055-s-0043-1768968.PMC10449566.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AORTA","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1768968","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study aimed to assess predictors of a composite endpoint (reoperation for aortic valve [AV] failure or aortic regurgitation [AR] grade ≥ 2) after reimplantation of the aortic valve (RAV) using the Valsalva graft.
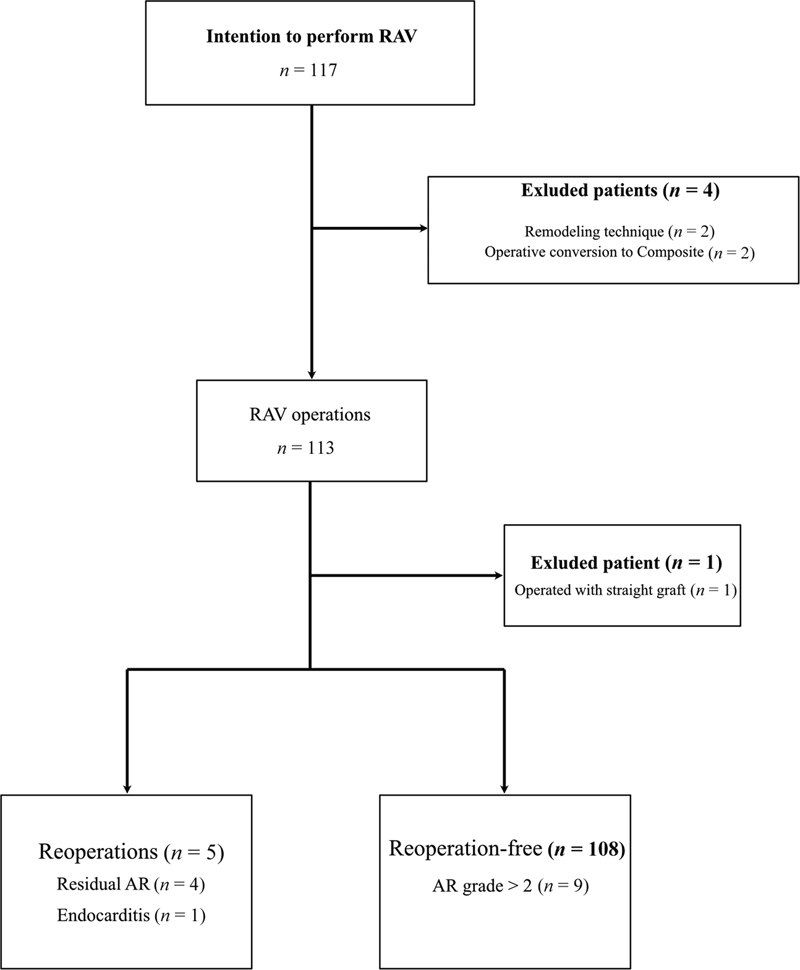
Methods: From 2012 to 2021, 112 patients underwent RAV in a single center. Clinical and echocardiographic data were collected retrospectively. Cox regression analysis was used to identify predictors of the composite endpoint. Kaplan-Meier methods were used for time-to-event analysis.
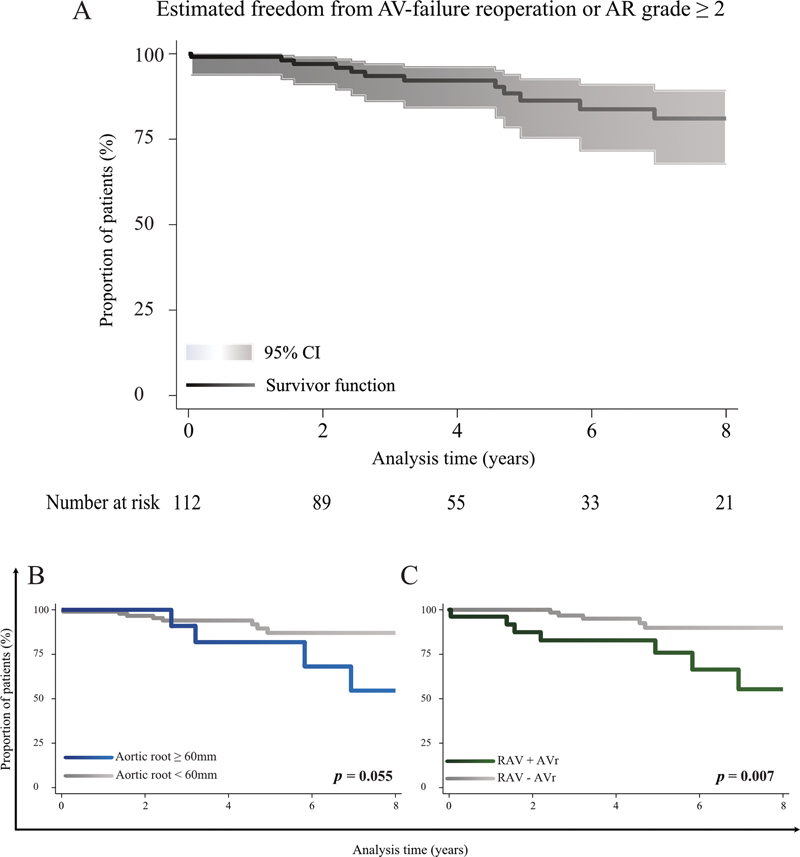
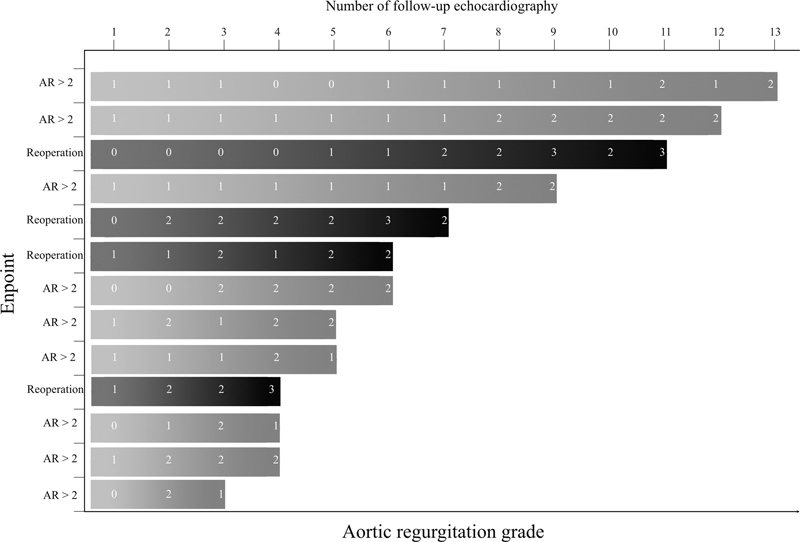
Results: Median (interquartile range) age was 52 years (44, 62). Nineteen patients (17%) were operated for acute Type A aortic dissection, and the remainder for aortic root aneurysm, 60 mm or larger in 12/112 (11%). Thirty-day mortality was 1/112 (1%). During follow-up, four patients (3.6%) were reoperated for AV failure, and another nine patients (8.1%) developed AR grade ≥ 2. Overall estimated freedom from reoperation or AR grade ≥ 2 was 87% (95% confidence interval: 76-93%) at 5 years. Significantly lower estimated 5-year freedom from the composite endpoint was found in cases with simultaneous aortic valve repair (AVr; 77 vs. 90%, p = 0.007) and nearly significant for large (≥ 6 cm) aortic root diameter (82 vs. 87%, p = 0.055). In Cox's analysis, aortic root diameter and simultaneous AVr were independent predictors for the composite endpoint.
Conclusion: Outcomes (survival, reoperation, freedom from AR grade ≥ 2) with RAV were good up to 11-year follow-up. Larger aortic root diameter and simultaneous AVr were identified as predictors for reoperation or AR grade ≥ 2. Long-term follow-up remains necessary to confirm adequate AV function.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


