Benjamin N Schmeusser, Tad A Manalo, Yuan Liu, Yash B Shah, Adil Ali, Manuel Armas-Phan, Dattatraya H Patil, Reza Nabavizadeh, Kenneth Ogan, Viraj A Master
{"title":"Mayo Adhesive Probability Score Does Not Have Prognostic Ability in Locally Advanced Renal Cell Carcinoma.","authors":"Benjamin N Schmeusser, Tad A Manalo, Yuan Liu, Yash B Shah, Adil Ali, Manuel Armas-Phan, Dattatraya H Patil, Reza Nabavizadeh, Kenneth Ogan, Viraj A Master","doi":"10.15586/jkcvhl.v10i1.269","DOIUrl":null,"url":null,"abstract":"<p><p>Nephrectomy remains standard treatment for renal cell carcinoma (RCC). The Mayo Adhesive Probability (MAP) score is predictive of adherent perinephric fat and associated surgical complexity, and is determined by assessing perinephric fat and stranding. MAP has additionally predicted progression-free survival (PFS), though primarily reported in stage T1-T2 RCC. Here, we examine MAP's ability to predict overall survival (OS) and PFS in T3-T4 RCC. From our prospectively maintained RCC database, patients that underwent radical nephrectomy (2009-2016) with available abdominal imaging (<90 days preop) and T3/T4 RCC underwent MAP scoring. Survival analyses were conducted with MAP scores as individual (0-5) and dichotomized (0-3 vs 4-5) using Kaplan-Meier method. Multivariable Cox proportional hazard regression models for PFS and OS were built with backward elimination. 141 patients were included. 134 (95%) and 7 (5%) had pT3 and pT4 disease, respectively. 46.1% of patients had an inferior vena cava thrombus. Mean MAP score was 3.22±1.52, with 75 (53%) patients having a score between 0-3 and 66 (47%) having a score of 4-5. Both male gender (p=0.006) and clear cell histology (p=0.012) were associated with increased MAP scores. On Kaplan-Meier and multivariable analysis, no significant associations were identified between MAP and PFS (HR=1.01, 95% CI 0.85-1.20, p=0.93) or OS (HR=1.01, 95% CI 0.84-1.21, p=0.917). In this cohort of patients with locally advanced RCC, high MAP scores were not predictive of worse PFS or OS.</p>","PeriodicalId":44291,"journal":{"name":"Journal of Kidney Cancer and VHL","volume":"10 1","pages":"19-25"},"PeriodicalIF":1.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10036918/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Kidney Cancer and VHL","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15586/jkcvhl.v10i1.269","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
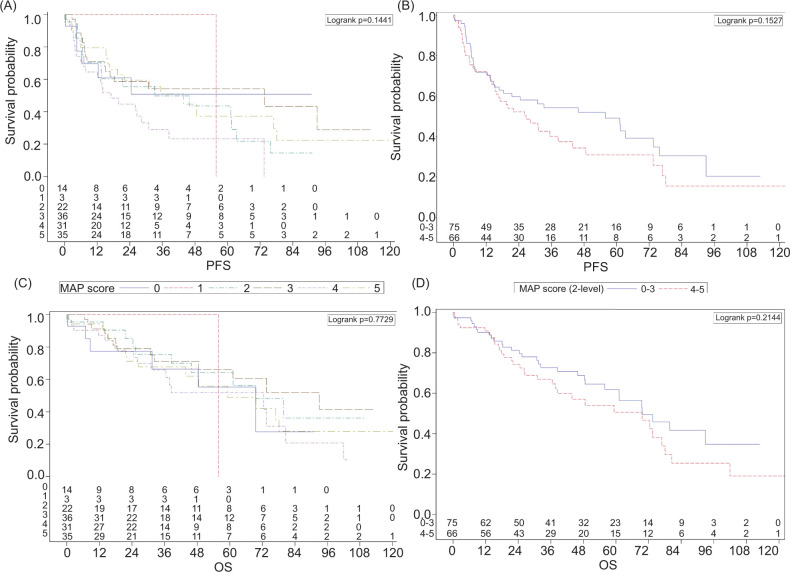
Nephrectomy remains standard treatment for renal cell carcinoma (RCC). The Mayo Adhesive Probability (MAP) score is predictive of adherent perinephric fat and associated surgical complexity, and is determined by assessing perinephric fat and stranding. MAP has additionally predicted progression-free survival (PFS), though primarily reported in stage T1-T2 RCC. Here, we examine MAP's ability to predict overall survival (OS) and PFS in T3-T4 RCC. From our prospectively maintained RCC database, patients that underwent radical nephrectomy (2009-2016) with available abdominal imaging (<90 days preop) and T3/T4 RCC underwent MAP scoring. Survival analyses were conducted with MAP scores as individual (0-5) and dichotomized (0-3 vs 4-5) using Kaplan-Meier method. Multivariable Cox proportional hazard regression models for PFS and OS were built with backward elimination. 141 patients were included. 134 (95%) and 7 (5%) had pT3 and pT4 disease, respectively. 46.1% of patients had an inferior vena cava thrombus. Mean MAP score was 3.22±1.52, with 75 (53%) patients having a score between 0-3 and 66 (47%) having a score of 4-5. Both male gender (p=0.006) and clear cell histology (p=0.012) were associated with increased MAP scores. On Kaplan-Meier and multivariable analysis, no significant associations were identified between MAP and PFS (HR=1.01, 95% CI 0.85-1.20, p=0.93) or OS (HR=1.01, 95% CI 0.84-1.21, p=0.917). In this cohort of patients with locally advanced RCC, high MAP scores were not predictive of worse PFS or OS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


