Yihong Deng, Eric C Polley, Joshua D Wallach, Jeph Herrin, Joseph S Ross, Rozalina G McCoy
{"title":"使用真实世界数据比较二线降血糖药物治疗的有效性:目标试验的模拟。","authors":"Yihong Deng, Eric C Polley, Joshua D Wallach, Jeph Herrin, Joseph S Ross, Rozalina G McCoy","doi":"10.1136/bmjmed-2022-000419","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To build on the recently completed GRADE (Glycemia Reduction Approaches in Diabetes: A Comparative Effectiveness Study) randomised trial examining the comparative effectiveness of second line glucose lowering drugs in achieving and maintaining glycaemic control in adults with type 2 diabetes.</p><p><strong>Design: </strong>Emulation of a target trial.</p><p><strong>Setting: </strong>Medical and pharmacy claims data from the OptumLabs Data Warehouse, a de-identified US national dataset of beneficiaries of commercially insured and Medicare Advantage plans, 29 March 2013 to 30 June 2021.</p><p><strong>Participants: </strong>Adults (≥18 years) with type 2 diabetes who first started taking glimepiride, sitagliptin, liraglutide, insulin glargine, or canagliflozin between 29 March 2013 and 30 June 2021. Participants were treatment naive or were receiving metformin monotherapy at the time of starting the study drug.</p><p><strong>Main outcome measures: </strong>The main outcomes were time to primary and secondary metabolic failure of the assigned treatment, calculated as days to haemoglobin A<sub>1c</sub> levels of ≥7.0% and >7.5%, respectively. Secondary metabolic, cardiovascular, and microvascular outcomes were analysed as specified in the GRADE statistical analysis plan. Propensity scores were estimated with the gradient boosting method, and inverse propensity score weighting was used to emulate randomisation to the treatment groups, which were then compared with Cox proportional hazards regression.</p><p><strong>Results: </strong>The study cohort included participants starting treatment with glimepiride (n=20 511), liraglutide (n=5569), sitagliptin (n=13 039), insulin glargine (n=7262), and canagliflozin (n=5290). The insulin glargine arm was excluded because of insufficient control of confounding. Median times to primary metabolic failure were 439 (95% confidence interval 400 to 489) days in the canagliflozin arm, 439 (426 to 453) days in the glimepiride arm, 624 (567 to 731) days in the liraglutide arm, and 461 (442 to 482) days in the sitagliptin arm. Median time to secondary metabolic failure was also longest in the liraglutide arm. Adults receiving liraglutide had the lowest one year cumulative incidence rate of primary metabolic failure (0.37, 95% confidence interval 0.35 to 0.40) followed by sitagliptin (0.44, 0.43 to 0.45), glimepiride (0.45, 0.44 to 0.45), and canagliflozin (0.46, 0.44 to 0.48). Similarly, the one year cumulative incidence rate of secondary metabolic failure was 0.27 (0.25 to 0.29) in the canagliflozin arm, 0.28 (0.27 to 0.29) in the glimepiride arm, 0.23 (0.21 to 0.26) in the liraglutide arm, and 0.28 (0.27 to 0.29) in the sitagliptin arm. No differences were observed between the study arms in the rates of microvascular and macrovascular complications.</p><p><strong>Conclusions: </strong>In this target trial emulation of an expanded GRADE study framework, liraglutide was more effective in achieving and maintaining glycaemic control as a second line glucose lowering drug than canagliflozin, sitagliptin, or glimepiride.</p>","PeriodicalId":72433,"journal":{"name":"BMJ medicine","volume":"2 1","pages":"e000419"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/12/c0/bmjmed-2022-000419.PMC10414064.pdf","citationCount":"1","resultStr":"{\"title\":\"Comparative effectiveness of second line glucose lowering drug treatments using real world data: emulation of a target trial.\",\"authors\":\"Yihong Deng, Eric C Polley, Joshua D Wallach, Jeph Herrin, Joseph S Ross, Rozalina G McCoy\",\"doi\":\"10.1136/bmjmed-2022-000419\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To build on the recently completed GRADE (Glycemia Reduction Approaches in Diabetes: A Comparative Effectiveness Study) randomised trial examining the comparative effectiveness of second line glucose lowering drugs in achieving and maintaining glycaemic control in adults with type 2 diabetes.</p><p><strong>Design: </strong>Emulation of a target trial.</p><p><strong>Setting: </strong>Medical and pharmacy claims data from the OptumLabs Data Warehouse, a de-identified US national dataset of beneficiaries of commercially insured and Medicare Advantage plans, 29 March 2013 to 30 June 2021.</p><p><strong>Participants: </strong>Adults (≥18 years) with type 2 diabetes who first started taking glimepiride, sitagliptin, liraglutide, insulin glargine, or canagliflozin between 29 March 2013 and 30 June 2021. Participants were treatment naive or were receiving metformin monotherapy at the time of starting the study drug.</p><p><strong>Main outcome measures: </strong>The main outcomes were time to primary and secondary metabolic failure of the assigned treatment, calculated as days to haemoglobin A<sub>1c</sub> levels of ≥7.0% and >7.5%, respectively. Secondary metabolic, cardiovascular, and microvascular outcomes were analysed as specified in the GRADE statistical analysis plan. Propensity scores were estimated with the gradient boosting method, and inverse propensity score weighting was used to emulate randomisation to the treatment groups, which were then compared with Cox proportional hazards regression.</p><p><strong>Results: </strong>The study cohort included participants starting treatment with glimepiride (n=20 511), liraglutide (n=5569), sitagliptin (n=13 039), insulin glargine (n=7262), and canagliflozin (n=5290). The insulin glargine arm was excluded because of insufficient control of confounding. Median times to primary metabolic failure were 439 (95% confidence interval 400 to 489) days in the canagliflozin arm, 439 (426 to 453) days in the glimepiride arm, 624 (567 to 731) days in the liraglutide arm, and 461 (442 to 482) days in the sitagliptin arm. Median time to secondary metabolic failure was also longest in the liraglutide arm. Adults receiving liraglutide had the lowest one year cumulative incidence rate of primary metabolic failure (0.37, 95% confidence interval 0.35 to 0.40) followed by sitagliptin (0.44, 0.43 to 0.45), glimepiride (0.45, 0.44 to 0.45), and canagliflozin (0.46, 0.44 to 0.48). Similarly, the one year cumulative incidence rate of secondary metabolic failure was 0.27 (0.25 to 0.29) in the canagliflozin arm, 0.28 (0.27 to 0.29) in the glimepiride arm, 0.23 (0.21 to 0.26) in the liraglutide arm, and 0.28 (0.27 to 0.29) in the sitagliptin arm. No differences were observed between the study arms in the rates of microvascular and macrovascular complications.</p><p><strong>Conclusions: </strong>In this target trial emulation of an expanded GRADE study framework, liraglutide was more effective in achieving and maintaining glycaemic control as a second line glucose lowering drug than canagliflozin, sitagliptin, or glimepiride.</p>\",\"PeriodicalId\":72433,\"journal\":{\"name\":\"BMJ medicine\",\"volume\":\"2 1\",\"pages\":\"e000419\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-08-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/12/c0/bmjmed-2022-000419.PMC10414064.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjmed-2022-000419\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjmed-2022-000419","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Comparative effectiveness of second line glucose lowering drug treatments using real world data: emulation of a target trial.
Objective: To build on the recently completed GRADE (Glycemia Reduction Approaches in Diabetes: A Comparative Effectiveness Study) randomised trial examining the comparative effectiveness of second line glucose lowering drugs in achieving and maintaining glycaemic control in adults with type 2 diabetes.
Design: Emulation of a target trial.
Setting: Medical and pharmacy claims data from the OptumLabs Data Warehouse, a de-identified US national dataset of beneficiaries of commercially insured and Medicare Advantage plans, 29 March 2013 to 30 June 2021.
Participants: Adults (≥18 years) with type 2 diabetes who first started taking glimepiride, sitagliptin, liraglutide, insulin glargine, or canagliflozin between 29 March 2013 and 30 June 2021. Participants were treatment naive or were receiving metformin monotherapy at the time of starting the study drug.
Main outcome measures: The main outcomes were time to primary and secondary metabolic failure of the assigned treatment, calculated as days to haemoglobin A1c levels of ≥7.0% and >7.5%, respectively. Secondary metabolic, cardiovascular, and microvascular outcomes were analysed as specified in the GRADE statistical analysis plan. Propensity scores were estimated with the gradient boosting method, and inverse propensity score weighting was used to emulate randomisation to the treatment groups, which were then compared with Cox proportional hazards regression.
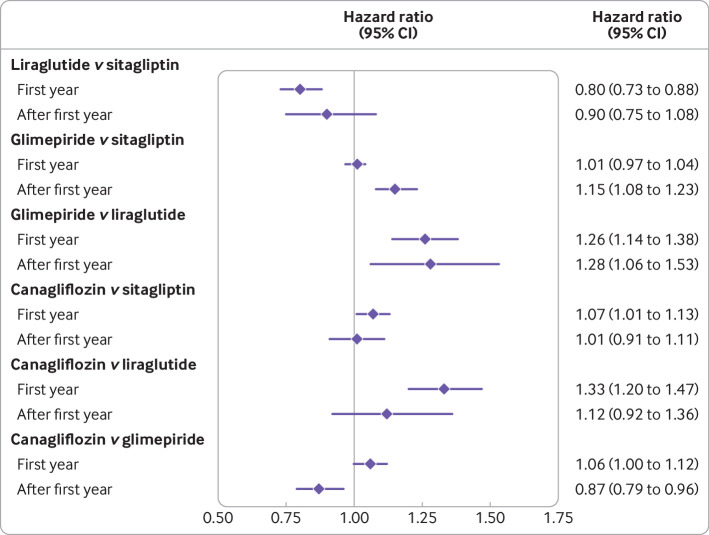
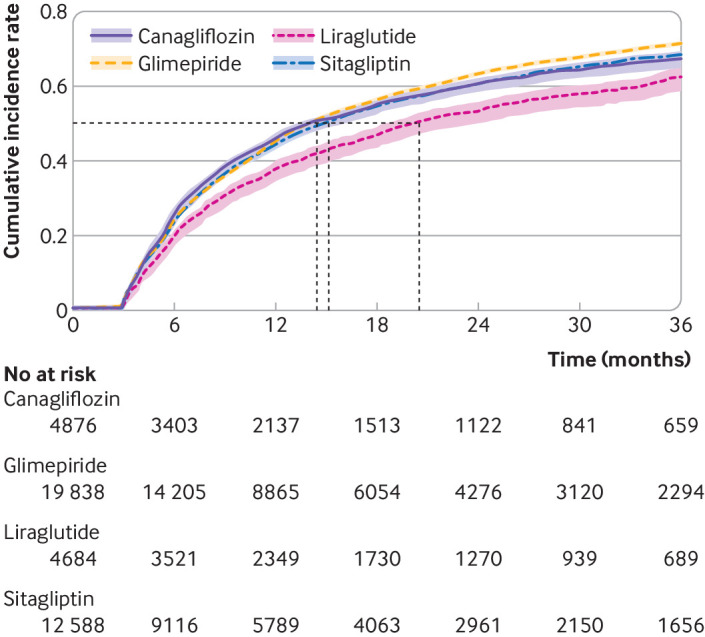
Results: The study cohort included participants starting treatment with glimepiride (n=20 511), liraglutide (n=5569), sitagliptin (n=13 039), insulin glargine (n=7262), and canagliflozin (n=5290). The insulin glargine arm was excluded because of insufficient control of confounding. Median times to primary metabolic failure were 439 (95% confidence interval 400 to 489) days in the canagliflozin arm, 439 (426 to 453) days in the glimepiride arm, 624 (567 to 731) days in the liraglutide arm, and 461 (442 to 482) days in the sitagliptin arm. Median time to secondary metabolic failure was also longest in the liraglutide arm. Adults receiving liraglutide had the lowest one year cumulative incidence rate of primary metabolic failure (0.37, 95% confidence interval 0.35 to 0.40) followed by sitagliptin (0.44, 0.43 to 0.45), glimepiride (0.45, 0.44 to 0.45), and canagliflozin (0.46, 0.44 to 0.48). Similarly, the one year cumulative incidence rate of secondary metabolic failure was 0.27 (0.25 to 0.29) in the canagliflozin arm, 0.28 (0.27 to 0.29) in the glimepiride arm, 0.23 (0.21 to 0.26) in the liraglutide arm, and 0.28 (0.27 to 0.29) in the sitagliptin arm. No differences were observed between the study arms in the rates of microvascular and macrovascular complications.
Conclusions: In this target trial emulation of an expanded GRADE study framework, liraglutide was more effective in achieving and maintaining glycaemic control as a second line glucose lowering drug than canagliflozin, sitagliptin, or glimepiride.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


