Keith Owen Yeates, Karen M Barlow, Bruce Wright, Ken Tang, Olesya Barrett, Edward Berdusco, Amanda M Black, Brenda Clark, Alf Conradi, Heather Godfrey, Ashley T Kolstad, Anh Ly, Angelo Mikrogianakis, Ross Purser, Kathryn Schneider, Antonia S Stang, Roger Zemek, Jennifer D Zwicker, David W Johnson
{"title":"实施儿科脑震荡急性护理临床路径对医疗保健的影响:阶梯式楔形聚类随机试验","authors":"Keith Owen Yeates, Karen M Barlow, Bruce Wright, Ken Tang, Olesya Barrett, Edward Berdusco, Amanda M Black, Brenda Clark, Alf Conradi, Heather Godfrey, Ashley T Kolstad, Anh Ly, Angelo Mikrogianakis, Ross Purser, Kathryn Schneider, Antonia S Stang, Roger Zemek, Jennifer D Zwicker, David W Johnson","doi":"10.1007/s43678-023-00530-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To test the effects of actively implementing a clinical pathway for acute care of pediatric concussion on health care utilization and costs.</p><p><strong>Methods: </strong>Stepped wedge, cluster randomized trial of a clinical pathway, conducted in 5 emergency departments (ED) in Alberta, Canada from February 1 to November 30, 2019. The clinical pathway emphasized standardized assessment of risk for persistent symptoms, provision of consistent information to patients and families, and referral for outpatient follow-up. De-identified administrative data measured 6 outcomes: ED return visits; outpatient follow-up visits; length of ED stay, including total time, time from triage to physician initial assessment, and time from physician initial assessment to disposition; and total physician claims in an episode of care.</p><p><strong>Results: </strong>A total of 2878 unique patients (1164 female, 1713 male) aged 5-17 years (median 11.00, IQR 8, 14) met case criteria. They completed 3009 visits to the 5 sites and 781 follow-up visits to outpatient care, constituting 2910 episodes of care. Implementation did not alter the likelihood of an ED return visit (OR 0.77, 95% CI 0.39, 1.52), but increased the likelihood of outpatient follow-up visits (OR 1.84, 95% CI 1.19, 2.85). Total length of ED stay was unchanged, but time from physician initial assessment to disposition decreased significantly (mean change - 23.76 min, 95% CI - 37.99, - 9.52). Total physician claims increased significantly at only 1 of 5 sites.</p><p><strong>Conclusions: </strong>Implementation of a clinical pathway in the ED increased outpatient follow-up and reduced the time from physician initial assessment to disposition, without increasing physician costs. Implementation of a clinical pathway can align acute care of pediatric concussion more closely with existing clinical practice guidelines while making care more efficient.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT05095012.</p>","PeriodicalId":55286,"journal":{"name":"Canadian Journal of Emergency Medicine","volume":"25 7","pages":"627-636"},"PeriodicalIF":2.0000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10333406/pdf/","citationCount":"0","resultStr":"{\"title\":\"Health care impact of implementing a clinical pathway for acute care of pediatric concussion: a stepped wedge, cluster randomised trial.\",\"authors\":\"Keith Owen Yeates, Karen M Barlow, Bruce Wright, Ken Tang, Olesya Barrett, Edward Berdusco, Amanda M Black, Brenda Clark, Alf Conradi, Heather Godfrey, Ashley T Kolstad, Anh Ly, Angelo Mikrogianakis, Ross Purser, Kathryn Schneider, Antonia S Stang, Roger Zemek, Jennifer D Zwicker, David W Johnson\",\"doi\":\"10.1007/s43678-023-00530-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To test the effects of actively implementing a clinical pathway for acute care of pediatric concussion on health care utilization and costs.</p><p><strong>Methods: </strong>Stepped wedge, cluster randomized trial of a clinical pathway, conducted in 5 emergency departments (ED) in Alberta, Canada from February 1 to November 30, 2019. The clinical pathway emphasized standardized assessment of risk for persistent symptoms, provision of consistent information to patients and families, and referral for outpatient follow-up. De-identified administrative data measured 6 outcomes: ED return visits; outpatient follow-up visits; length of ED stay, including total time, time from triage to physician initial assessment, and time from physician initial assessment to disposition; and total physician claims in an episode of care.</p><p><strong>Results: </strong>A total of 2878 unique patients (1164 female, 1713 male) aged 5-17 years (median 11.00, IQR 8, 14) met case criteria. They completed 3009 visits to the 5 sites and 781 follow-up visits to outpatient care, constituting 2910 episodes of care. Implementation did not alter the likelihood of an ED return visit (OR 0.77, 95% CI 0.39, 1.52), but increased the likelihood of outpatient follow-up visits (OR 1.84, 95% CI 1.19, 2.85). Total length of ED stay was unchanged, but time from physician initial assessment to disposition decreased significantly (mean change - 23.76 min, 95% CI - 37.99, - 9.52). Total physician claims increased significantly at only 1 of 5 sites.</p><p><strong>Conclusions: </strong>Implementation of a clinical pathway in the ED increased outpatient follow-up and reduced the time from physician initial assessment to disposition, without increasing physician costs. Implementation of a clinical pathway can align acute care of pediatric concussion more closely with existing clinical practice guidelines while making care more efficient.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT05095012.</p>\",\"PeriodicalId\":55286,\"journal\":{\"name\":\"Canadian Journal of Emergency Medicine\",\"volume\":\"25 7\",\"pages\":\"627-636\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10333406/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s43678-023-00530-1\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s43678-023-00530-1","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
目的:探讨积极实施儿童脑震荡急性护理临床路径对医疗服务利用和成本的影响。方法:2019年2月1日至11月30日,在加拿大阿尔伯塔省5个急诊科(ED)开展临床路径的楔形聚类随机试验。临床路径强调对持续症状的风险进行标准化评估,向患者和家属提供一致的信息,并转介门诊随访。去识别的行政数据测量了6个结果:ED回访;门诊随访;急诊科住院时间,包括总时间,从分诊到医生初步评估的时间,以及从医生初步评估到处置的时间;在一次护理中,医生的总索赔。结果:2878例患者(女性1164例,男性1713例)符合病例标准,年龄5-17岁(中位数11.00,IQR 8,14)。他们完成了对5个地点的3009次访问和781次门诊随访,共2910次护理。实施并没有改变急诊科复诊的可能性(OR 0.77, 95% CI 0.39, 1.52),但增加了门诊随访的可能性(OR 1.84, 95% CI 1.19, 2.85)。急诊科的总住院时间没有变化,但从医生最初评估到处置的时间显著减少(平均变化- 23.76分钟,95% CI - 37.99, - 9.52)。在5个站点中,只有1个站点的医生总索赔显著增加。结论:在急诊科实施临床路径增加了门诊随访,减少了从医生初步评估到处置的时间,而没有增加医生的成本。临床路径的实施可以使儿童脑震荡的急性护理更紧密地与现有的临床实践指南保持一致,同时提高护理效率。试验注册:ClinicalTrials.gov NCT05095012。
Health care impact of implementing a clinical pathway for acute care of pediatric concussion: a stepped wedge, cluster randomised trial.
Objectives: To test the effects of actively implementing a clinical pathway for acute care of pediatric concussion on health care utilization and costs.
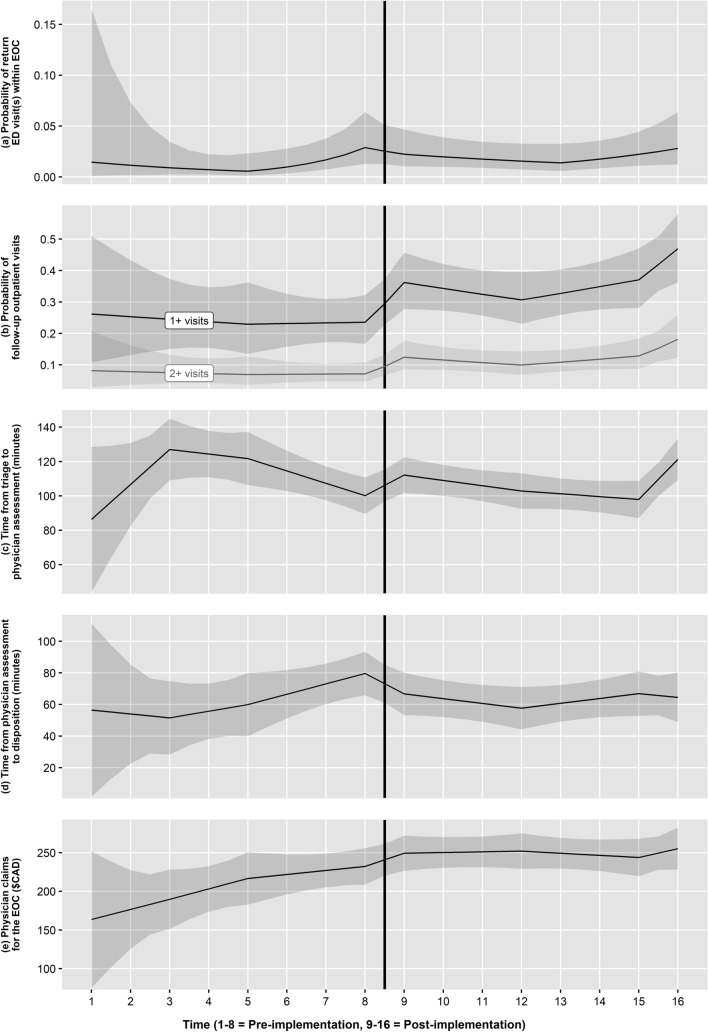
Methods: Stepped wedge, cluster randomized trial of a clinical pathway, conducted in 5 emergency departments (ED) in Alberta, Canada from February 1 to November 30, 2019. The clinical pathway emphasized standardized assessment of risk for persistent symptoms, provision of consistent information to patients and families, and referral for outpatient follow-up. De-identified administrative data measured 6 outcomes: ED return visits; outpatient follow-up visits; length of ED stay, including total time, time from triage to physician initial assessment, and time from physician initial assessment to disposition; and total physician claims in an episode of care.
Results: A total of 2878 unique patients (1164 female, 1713 male) aged 5-17 years (median 11.00, IQR 8, 14) met case criteria. They completed 3009 visits to the 5 sites and 781 follow-up visits to outpatient care, constituting 2910 episodes of care. Implementation did not alter the likelihood of an ED return visit (OR 0.77, 95% CI 0.39, 1.52), but increased the likelihood of outpatient follow-up visits (OR 1.84, 95% CI 1.19, 2.85). Total length of ED stay was unchanged, but time from physician initial assessment to disposition decreased significantly (mean change - 23.76 min, 95% CI - 37.99, - 9.52). Total physician claims increased significantly at only 1 of 5 sites.
Conclusions: Implementation of a clinical pathway in the ED increased outpatient follow-up and reduced the time from physician initial assessment to disposition, without increasing physician costs. Implementation of a clinical pathway can align acute care of pediatric concussion more closely with existing clinical practice guidelines while making care more efficient.
期刊介绍:
CJEM is a peer-reviewed journal owned by CAEP. CJEM is published every 2 months (January, March, May, July, September and November). CJEM presents articles of interest to emergency care providers in rural, urban or academic settings. Publishing services are provided by the Canadian Medical Association.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


