{"title":"酒精戒断伴震颤谵妄。","authors":"Courtney Schwebach, Amrita Vempati","doi":"10.21980/J8S35N","DOIUrl":null,"url":null,"abstract":"<p><strong>Audience: </strong>Emergency medicine (EM) residents (1<sup>st</sup> year and 2<sup>nd</sup> year levels), 4th year medical students and advanced practice providers.</p><p><strong>Introduction: </strong>Alcohol use has played a major role in causing significant morbidity and mortality for patients. In 2016, it was the 7th leading risk factor for deaths and disability-adjusted life years globally.1 Among heavy alcohol users admitted for hospital management, the incidence of alcohol withdrawal syndrome is estimated to be 1.9 to 6.7%.1 Alcohol withdrawal (AW) in the ED has been associated with increased use of critical care resources, and frequent ED visits for alcohol-related presentations have been associated with mortality rates that are about 1-4% when withdrawal progresses to delirium tremens (DTs).1 Patients with alcohol withdrawal can present in many different ways to the ED including anxiety, tachycardia, delirium tremens (DTs), seizures and severe autonomic dysfunction leading to severe sickness and death.2 Therefore, it is extremely important for an EM physician to recognize the signs of AW in patients and to manage the critically ill patients. In addition, Clinical Institute Withdrawal Assessment (CIWA) of alcohol was developed to assess severity of alcohol withdrawal in 1989.3 EM physicians should utilize CIWA to help determine the severity of AW.</p><p><strong>Educational objectives: </strong>By the end of the session, learner will be able to 1) discuss the causes of altered mental status, 2) utilize CIWA scoring system to quantify AW severity, 3) formulate appropriate treatment plan for AW by treating with benzodiazepine and escalating treatment appropriately, 4) treat electrolyte abnormalities by giving appropriate medications for hypokalemia and hypomagnesemia, and 5) discuss clinical progression and timing to AW.</p><p><strong>Educational methods: </strong>This session was conducted using high-fidelity simulation, which was immediately followed by an in-depth debriefing session. The session was run during first year EM resident intern orientation, and it was run during two consecutive years. There was a total of 32 EM residents who participated. There was a total of 16 residents who actively managed the patient while the other 16 were observers. Each session had four learners and was run twice in two separate rooms. There was one simulation instructor running the session and one simulation technician who acted as a nurse.</p><p><strong>Research methods: </strong>After the simulation and debriefing session was complete, an online survey was sent via surveymonkey.com to all the participants. The survey collected responses to the following questions: (1) the case was believable, (2) the case had right the amount of complexity (based on their Gestalt), (3) the case helped in improving medical knowledge and patient care, (4) the simulation environment gave me a real-life experience and, (5) the debriefing session after simulation helped improve my knowledge. The responses were collected using a Likert scale of 1 to 5 with 1 being \"Strongly disagree\" and 5 being \"Strongly agree.\"</p><p><strong>Results: </strong>There was a total of 15 respondents from both years. One hundred percent of them either agreed or strongly agreed that the case was beneficial in learning, in improving medical knowledge and in patient care. All of them found the post-session debrief to be very helpful. Two of them felt neutral about the case being realistic. The median response for questions 1, 3 and 5 is 5. The median response for questions 2 and 4 was 4. The range of responses for questions 1, 2, 3 and 5 was 4-5 while the range for question 4 was 3-5.</p><p><strong>Discussion: </strong>This high-fidelity simulation was a cost-effective and realistic way of educating learners on how to manage AW with DTs. Learners are forced to start with a broad differential for the patient who presents with AMS. As they recognize the cause of mental status, the patient quickly decompensates into developing severe agitation and autonomic dysfunction requiring learners to manage the patient and establish an airway. Learners found the case to be beneficial in learning the management of AW.</p><p><strong>Topics: </strong>Alcohol withdrawal, delirium tremens, agitation, altered mental status.</p>","PeriodicalId":73721,"journal":{"name":"Journal of education & teaching in emergency medicine","volume":"8 3","pages":"S1-S33"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10414982/pdf/","citationCount":"0","resultStr":"{\"title\":\"Alcohol Withdrawal with Delirium Tremens.\",\"authors\":\"Courtney Schwebach, Amrita Vempati\",\"doi\":\"10.21980/J8S35N\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Audience: </strong>Emergency medicine (EM) residents (1<sup>st</sup> year and 2<sup>nd</sup> year levels), 4th year medical students and advanced practice providers.</p><p><strong>Introduction: </strong>Alcohol use has played a major role in causing significant morbidity and mortality for patients. In 2016, it was the 7th leading risk factor for deaths and disability-adjusted life years globally.1 Among heavy alcohol users admitted for hospital management, the incidence of alcohol withdrawal syndrome is estimated to be 1.9 to 6.7%.1 Alcohol withdrawal (AW) in the ED has been associated with increased use of critical care resources, and frequent ED visits for alcohol-related presentations have been associated with mortality rates that are about 1-4% when withdrawal progresses to delirium tremens (DTs).1 Patients with alcohol withdrawal can present in many different ways to the ED including anxiety, tachycardia, delirium tremens (DTs), seizures and severe autonomic dysfunction leading to severe sickness and death.2 Therefore, it is extremely important for an EM physician to recognize the signs of AW in patients and to manage the critically ill patients. In addition, Clinical Institute Withdrawal Assessment (CIWA) of alcohol was developed to assess severity of alcohol withdrawal in 1989.3 EM physicians should utilize CIWA to help determine the severity of AW.</p><p><strong>Educational objectives: </strong>By the end of the session, learner will be able to 1) discuss the causes of altered mental status, 2) utilize CIWA scoring system to quantify AW severity, 3) formulate appropriate treatment plan for AW by treating with benzodiazepine and escalating treatment appropriately, 4) treat electrolyte abnormalities by giving appropriate medications for hypokalemia and hypomagnesemia, and 5) discuss clinical progression and timing to AW.</p><p><strong>Educational methods: </strong>This session was conducted using high-fidelity simulation, which was immediately followed by an in-depth debriefing session. The session was run during first year EM resident intern orientation, and it was run during two consecutive years. There was a total of 32 EM residents who participated. There was a total of 16 residents who actively managed the patient while the other 16 were observers. Each session had four learners and was run twice in two separate rooms. There was one simulation instructor running the session and one simulation technician who acted as a nurse.</p><p><strong>Research methods: </strong>After the simulation and debriefing session was complete, an online survey was sent via surveymonkey.com to all the participants. The survey collected responses to the following questions: (1) the case was believable, (2) the case had right the amount of complexity (based on their Gestalt), (3) the case helped in improving medical knowledge and patient care, (4) the simulation environment gave me a real-life experience and, (5) the debriefing session after simulation helped improve my knowledge. The responses were collected using a Likert scale of 1 to 5 with 1 being \\\"Strongly disagree\\\" and 5 being \\\"Strongly agree.\\\"</p><p><strong>Results: </strong>There was a total of 15 respondents from both years. One hundred percent of them either agreed or strongly agreed that the case was beneficial in learning, in improving medical knowledge and in patient care. All of them found the post-session debrief to be very helpful. Two of them felt neutral about the case being realistic. The median response for questions 1, 3 and 5 is 5. The median response for questions 2 and 4 was 4. The range of responses for questions 1, 2, 3 and 5 was 4-5 while the range for question 4 was 3-5.</p><p><strong>Discussion: </strong>This high-fidelity simulation was a cost-effective and realistic way of educating learners on how to manage AW with DTs. Learners are forced to start with a broad differential for the patient who presents with AMS. As they recognize the cause of mental status, the patient quickly decompensates into developing severe agitation and autonomic dysfunction requiring learners to manage the patient and establish an airway. Learners found the case to be beneficial in learning the management of AW.</p><p><strong>Topics: </strong>Alcohol withdrawal, delirium tremens, agitation, altered mental status.</p>\",\"PeriodicalId\":73721,\"journal\":{\"name\":\"Journal of education & teaching in emergency medicine\",\"volume\":\"8 3\",\"pages\":\"S1-S33\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10414982/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of education & teaching in emergency medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21980/J8S35N\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of education & teaching in emergency medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21980/J8S35N","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Audience: Emergency medicine (EM) residents (1st year and 2nd year levels), 4th year medical students and advanced practice providers.
Introduction: Alcohol use has played a major role in causing significant morbidity and mortality for patients. In 2016, it was the 7th leading risk factor for deaths and disability-adjusted life years globally.1 Among heavy alcohol users admitted for hospital management, the incidence of alcohol withdrawal syndrome is estimated to be 1.9 to 6.7%.1 Alcohol withdrawal (AW) in the ED has been associated with increased use of critical care resources, and frequent ED visits for alcohol-related presentations have been associated with mortality rates that are about 1-4% when withdrawal progresses to delirium tremens (DTs).1 Patients with alcohol withdrawal can present in many different ways to the ED including anxiety, tachycardia, delirium tremens (DTs), seizures and severe autonomic dysfunction leading to severe sickness and death.2 Therefore, it is extremely important for an EM physician to recognize the signs of AW in patients and to manage the critically ill patients. In addition, Clinical Institute Withdrawal Assessment (CIWA) of alcohol was developed to assess severity of alcohol withdrawal in 1989.3 EM physicians should utilize CIWA to help determine the severity of AW.
Educational objectives: By the end of the session, learner will be able to 1) discuss the causes of altered mental status, 2) utilize CIWA scoring system to quantify AW severity, 3) formulate appropriate treatment plan for AW by treating with benzodiazepine and escalating treatment appropriately, 4) treat electrolyte abnormalities by giving appropriate medications for hypokalemia and hypomagnesemia, and 5) discuss clinical progression and timing to AW.
Educational methods: This session was conducted using high-fidelity simulation, which was immediately followed by an in-depth debriefing session. The session was run during first year EM resident intern orientation, and it was run during two consecutive years. There was a total of 32 EM residents who participated. There was a total of 16 residents who actively managed the patient while the other 16 were observers. Each session had four learners and was run twice in two separate rooms. There was one simulation instructor running the session and one simulation technician who acted as a nurse.
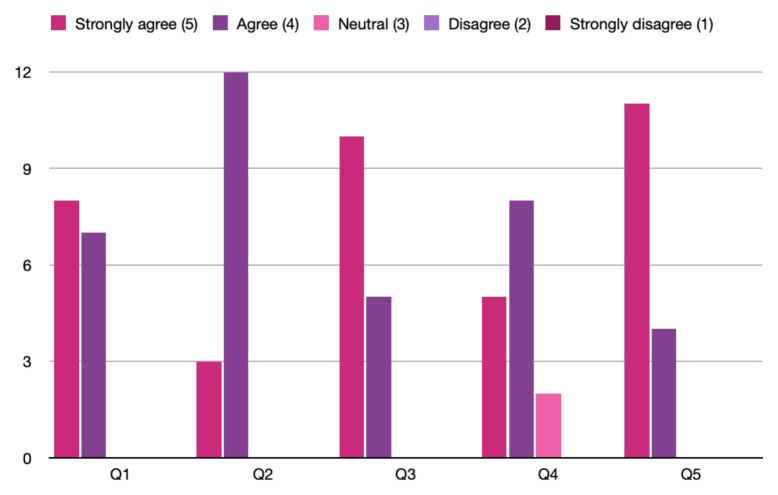
Research methods: After the simulation and debriefing session was complete, an online survey was sent via surveymonkey.com to all the participants. The survey collected responses to the following questions: (1) the case was believable, (2) the case had right the amount of complexity (based on their Gestalt), (3) the case helped in improving medical knowledge and patient care, (4) the simulation environment gave me a real-life experience and, (5) the debriefing session after simulation helped improve my knowledge. The responses were collected using a Likert scale of 1 to 5 with 1 being "Strongly disagree" and 5 being "Strongly agree."
Results: There was a total of 15 respondents from both years. One hundred percent of them either agreed or strongly agreed that the case was beneficial in learning, in improving medical knowledge and in patient care. All of them found the post-session debrief to be very helpful. Two of them felt neutral about the case being realistic. The median response for questions 1, 3 and 5 is 5. The median response for questions 2 and 4 was 4. The range of responses for questions 1, 2, 3 and 5 was 4-5 while the range for question 4 was 3-5.
Discussion: This high-fidelity simulation was a cost-effective and realistic way of educating learners on how to manage AW with DTs. Learners are forced to start with a broad differential for the patient who presents with AMS. As they recognize the cause of mental status, the patient quickly decompensates into developing severe agitation and autonomic dysfunction requiring learners to manage the patient and establish an airway. Learners found the case to be beneficial in learning the management of AW.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


