{"title":"急性肺水肿与NSTEMI。","authors":"Ashley Pilgrim","doi":"10.21980/J8CW67","DOIUrl":null,"url":null,"abstract":"<p><strong>Audience: </strong>Emergency medicine residents and medical students on emergency medicine rotation.</p><p><strong>Introduction: </strong>Acute pulmonary edema is a common and potentially fatal presentation in the emergency department. More than 1 million patients are admitted annually with a diagnosis of pulmonary edema secondary to cardiac causes.1 Pulmonary edema is broadly split into two main categories: cardiogenic and noncardiogenic. Cardiogenic pulmonary edema is characterized by acute dyspnea caused by the accumulation of fluid within the lung's interstitial and/or alveolar spaces, which is the result of acutely elevated cardiac filling pressures.2 Noncardiogenic pulmonary edema is characterized by fluid accumulation within the alveolar space in the absence of elevated pulmonary capillary wedge pressure.2 These patients often present critically ill, and rapid identification and aggressive management is paramount in caring for patients with pulmonary edema. Dyspnea is the most common presentation with a sensitivity of 89% but a low specificity of 51%.3 Workup of pulmonary edema often includes laboratory testing, electrocardiogram (EKG), chest x-ray (CXR), and often bedside ultrasound (US) and echocardiography.4 Pulmonary edema management depends on the etiology but is often focused on preload and afterload reduction. Diuretics, nitrates, and optimizing ventilatory support through non-invasive and invasive strategies are the mainstay of treatment.</p><p><strong>Educational objectives: </strong>At the end of this practice oral boards case, the learner will:1) recognize unstable vital signs (VS) and intervene to stabilize ventilation and oxygenation, 2) demonstrate the ability to obtain a complete medical history including the important characteristics of chest pain, 3) demonstrate an appropriate exam on a patient, 4) order the appropriate evaluation studies for a patient with complaints of dyspnea, 5) interpret the results of diagnostic evaluation and diagnose Non- ST elevation myocardial infarction (NSTEMI) and pulmonary edema, 6) order appropriate management of pulmonary edema and NSTEMI, and 6) demonstrate effective communication with patient and family members.</p><p><strong>Educational methods: </strong>Practice oral boards.</p><p><strong>Research methods: </strong>Immediate Feedback was solicited from the learners and observers participating in the case both by verbal discussion and completion of a rating for the case following the debriefing. The efficacy of the educational content was assessed by comparing scoring measures across residents based on the training year. Scoring measures of the American College of Graduate Medical Education (ACGME) core competencies were performed using a scale from 1 - 8, 1-4 being unacceptable performance and 5 - 8 being acceptable. Efficacy was assumed based on full completion of the case by the residents who acted as practice oral board candidates, and a debriefing session followed to discuss the key components of the case.</p><p><strong>Results: </strong>This case was presented to twelve Emergency Medicine Residents, seven PGY 1 and five PGY 2 at a relatively new residency program. The overall average score for the residents was 5.62. The PGY 1 Residents' average on the case was 5.56, and the average for the PGY 2 Residents was slightly better at 5.70. The slight improvement noted by the PGY 2 Residents is likely attributable to more clinical experience; however, both classes did not have any prior exposure to the oral board format until this simulated experience. Six residents completed all critical actions in the case. Of those who missed a critical action, failing to diagnose NSTEMI and consulting cardiology were the most common. All learners found educational value in the case with an overall rating of 4.83 (1-5 Likert scale, 5 being excellent).</p><p><strong>Discussion: </strong>Acute pulmonary edema and NSTEMI are common diagnoses that will be frequently encountered for most emergency physicians. This case highlights the need for early identification and aggressive management of the patient presenting with respiratory distress. The differential for respiratory distress is large, but most learners were able to quickly identify pulmonary edema based on the exam findings of jugular vein distention (JVD), rales, and lower extremity edema. Most learners quickly escalated to a non-rebreather mask and ultimately to BPAP (bilevel positive airway pressure) without requesting to intubate the patient. There was notable variation in the approach to administering nitrates, but most ordered an intravenous (IV) nitroglycerin (NTG) drip and requested pharmacy assistance in dosing. Diuretics were ordered by all the learners, but some were hesitant to start early because they felt the effect would be delayed. Some of the residents did not identify ischemic changes on the EKG at first glance but did request to review a second time when the troponin result was positive. All residents gave aspirin after noting the positive troponin, but not all were able to make a clear diagnosis of NSTEMI or consult cardiology. Although the case was relatively straightforward, residents enjoyed early diagnosis and aggressive management of the patient with impending respiratory failure. Many residents are asking for an ultrasound early in the workup of this patient presenting in respiratory distress. Although not a critical action in this case, it highlights the emphasis placed on ultrasonography in the current emergency medicine curriculum.</p><p><strong>Topics: </strong>Pulmonary Edema, Cardiovascular emergencies, NSTEMI.</p>","PeriodicalId":73721,"journal":{"name":"Journal of education & teaching in emergency medicine","volume":"8 3","pages":"O1-O32"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10414976/pdf/","citationCount":"1","resultStr":"{\"title\":\"Acute Pulmonary Edema and NSTEMI.\",\"authors\":\"Ashley Pilgrim\",\"doi\":\"10.21980/J8CW67\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Audience: </strong>Emergency medicine residents and medical students on emergency medicine rotation.</p><p><strong>Introduction: </strong>Acute pulmonary edema is a common and potentially fatal presentation in the emergency department. More than 1 million patients are admitted annually with a diagnosis of pulmonary edema secondary to cardiac causes.1 Pulmonary edema is broadly split into two main categories: cardiogenic and noncardiogenic. Cardiogenic pulmonary edema is characterized by acute dyspnea caused by the accumulation of fluid within the lung's interstitial and/or alveolar spaces, which is the result of acutely elevated cardiac filling pressures.2 Noncardiogenic pulmonary edema is characterized by fluid accumulation within the alveolar space in the absence of elevated pulmonary capillary wedge pressure.2 These patients often present critically ill, and rapid identification and aggressive management is paramount in caring for patients with pulmonary edema. Dyspnea is the most common presentation with a sensitivity of 89% but a low specificity of 51%.3 Workup of pulmonary edema often includes laboratory testing, electrocardiogram (EKG), chest x-ray (CXR), and often bedside ultrasound (US) and echocardiography.4 Pulmonary edema management depends on the etiology but is often focused on preload and afterload reduction. Diuretics, nitrates, and optimizing ventilatory support through non-invasive and invasive strategies are the mainstay of treatment.</p><p><strong>Educational objectives: </strong>At the end of this practice oral boards case, the learner will:1) recognize unstable vital signs (VS) and intervene to stabilize ventilation and oxygenation, 2) demonstrate the ability to obtain a complete medical history including the important characteristics of chest pain, 3) demonstrate an appropriate exam on a patient, 4) order the appropriate evaluation studies for a patient with complaints of dyspnea, 5) interpret the results of diagnostic evaluation and diagnose Non- ST elevation myocardial infarction (NSTEMI) and pulmonary edema, 6) order appropriate management of pulmonary edema and NSTEMI, and 6) demonstrate effective communication with patient and family members.</p><p><strong>Educational methods: </strong>Practice oral boards.</p><p><strong>Research methods: </strong>Immediate Feedback was solicited from the learners and observers participating in the case both by verbal discussion and completion of a rating for the case following the debriefing. The efficacy of the educational content was assessed by comparing scoring measures across residents based on the training year. Scoring measures of the American College of Graduate Medical Education (ACGME) core competencies were performed using a scale from 1 - 8, 1-4 being unacceptable performance and 5 - 8 being acceptable. Efficacy was assumed based on full completion of the case by the residents who acted as practice oral board candidates, and a debriefing session followed to discuss the key components of the case.</p><p><strong>Results: </strong>This case was presented to twelve Emergency Medicine Residents, seven PGY 1 and five PGY 2 at a relatively new residency program. The overall average score for the residents was 5.62. The PGY 1 Residents' average on the case was 5.56, and the average for the PGY 2 Residents was slightly better at 5.70. The slight improvement noted by the PGY 2 Residents is likely attributable to more clinical experience; however, both classes did not have any prior exposure to the oral board format until this simulated experience. Six residents completed all critical actions in the case. Of those who missed a critical action, failing to diagnose NSTEMI and consulting cardiology were the most common. All learners found educational value in the case with an overall rating of 4.83 (1-5 Likert scale, 5 being excellent).</p><p><strong>Discussion: </strong>Acute pulmonary edema and NSTEMI are common diagnoses that will be frequently encountered for most emergency physicians. This case highlights the need for early identification and aggressive management of the patient presenting with respiratory distress. The differential for respiratory distress is large, but most learners were able to quickly identify pulmonary edema based on the exam findings of jugular vein distention (JVD), rales, and lower extremity edema. Most learners quickly escalated to a non-rebreather mask and ultimately to BPAP (bilevel positive airway pressure) without requesting to intubate the patient. There was notable variation in the approach to administering nitrates, but most ordered an intravenous (IV) nitroglycerin (NTG) drip and requested pharmacy assistance in dosing. Diuretics were ordered by all the learners, but some were hesitant to start early because they felt the effect would be delayed. Some of the residents did not identify ischemic changes on the EKG at first glance but did request to review a second time when the troponin result was positive. All residents gave aspirin after noting the positive troponin, but not all were able to make a clear diagnosis of NSTEMI or consult cardiology. Although the case was relatively straightforward, residents enjoyed early diagnosis and aggressive management of the patient with impending respiratory failure. Many residents are asking for an ultrasound early in the workup of this patient presenting in respiratory distress. Although not a critical action in this case, it highlights the emphasis placed on ultrasonography in the current emergency medicine curriculum.</p><p><strong>Topics: </strong>Pulmonary Edema, Cardiovascular emergencies, NSTEMI.</p>\",\"PeriodicalId\":73721,\"journal\":{\"name\":\"Journal of education & teaching in emergency medicine\",\"volume\":\"8 3\",\"pages\":\"O1-O32\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10414976/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of education & teaching in emergency medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21980/J8CW67\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of education & teaching in emergency medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21980/J8CW67","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Audience: Emergency medicine residents and medical students on emergency medicine rotation.
Introduction: Acute pulmonary edema is a common and potentially fatal presentation in the emergency department. More than 1 million patients are admitted annually with a diagnosis of pulmonary edema secondary to cardiac causes.1 Pulmonary edema is broadly split into two main categories: cardiogenic and noncardiogenic. Cardiogenic pulmonary edema is characterized by acute dyspnea caused by the accumulation of fluid within the lung's interstitial and/or alveolar spaces, which is the result of acutely elevated cardiac filling pressures.2 Noncardiogenic pulmonary edema is characterized by fluid accumulation within the alveolar space in the absence of elevated pulmonary capillary wedge pressure.2 These patients often present critically ill, and rapid identification and aggressive management is paramount in caring for patients with pulmonary edema. Dyspnea is the most common presentation with a sensitivity of 89% but a low specificity of 51%.3 Workup of pulmonary edema often includes laboratory testing, electrocardiogram (EKG), chest x-ray (CXR), and often bedside ultrasound (US) and echocardiography.4 Pulmonary edema management depends on the etiology but is often focused on preload and afterload reduction. Diuretics, nitrates, and optimizing ventilatory support through non-invasive and invasive strategies are the mainstay of treatment.
Educational objectives: At the end of this practice oral boards case, the learner will:1) recognize unstable vital signs (VS) and intervene to stabilize ventilation and oxygenation, 2) demonstrate the ability to obtain a complete medical history including the important characteristics of chest pain, 3) demonstrate an appropriate exam on a patient, 4) order the appropriate evaluation studies for a patient with complaints of dyspnea, 5) interpret the results of diagnostic evaluation and diagnose Non- ST elevation myocardial infarction (NSTEMI) and pulmonary edema, 6) order appropriate management of pulmonary edema and NSTEMI, and 6) demonstrate effective communication with patient and family members.
Educational methods: Practice oral boards.
Research methods: Immediate Feedback was solicited from the learners and observers participating in the case both by verbal discussion and completion of a rating for the case following the debriefing. The efficacy of the educational content was assessed by comparing scoring measures across residents based on the training year. Scoring measures of the American College of Graduate Medical Education (ACGME) core competencies were performed using a scale from 1 - 8, 1-4 being unacceptable performance and 5 - 8 being acceptable. Efficacy was assumed based on full completion of the case by the residents who acted as practice oral board candidates, and a debriefing session followed to discuss the key components of the case.
Results: This case was presented to twelve Emergency Medicine Residents, seven PGY 1 and five PGY 2 at a relatively new residency program. The overall average score for the residents was 5.62. The PGY 1 Residents' average on the case was 5.56, and the average for the PGY 2 Residents was slightly better at 5.70. The slight improvement noted by the PGY 2 Residents is likely attributable to more clinical experience; however, both classes did not have any prior exposure to the oral board format until this simulated experience. Six residents completed all critical actions in the case. Of those who missed a critical action, failing to diagnose NSTEMI and consulting cardiology were the most common. All learners found educational value in the case with an overall rating of 4.83 (1-5 Likert scale, 5 being excellent).
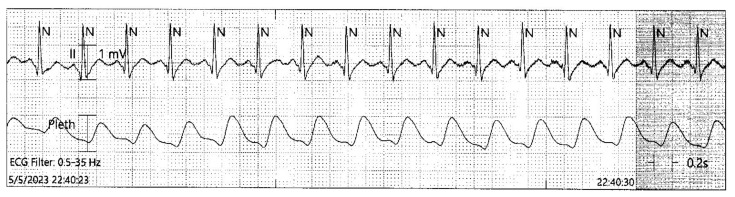
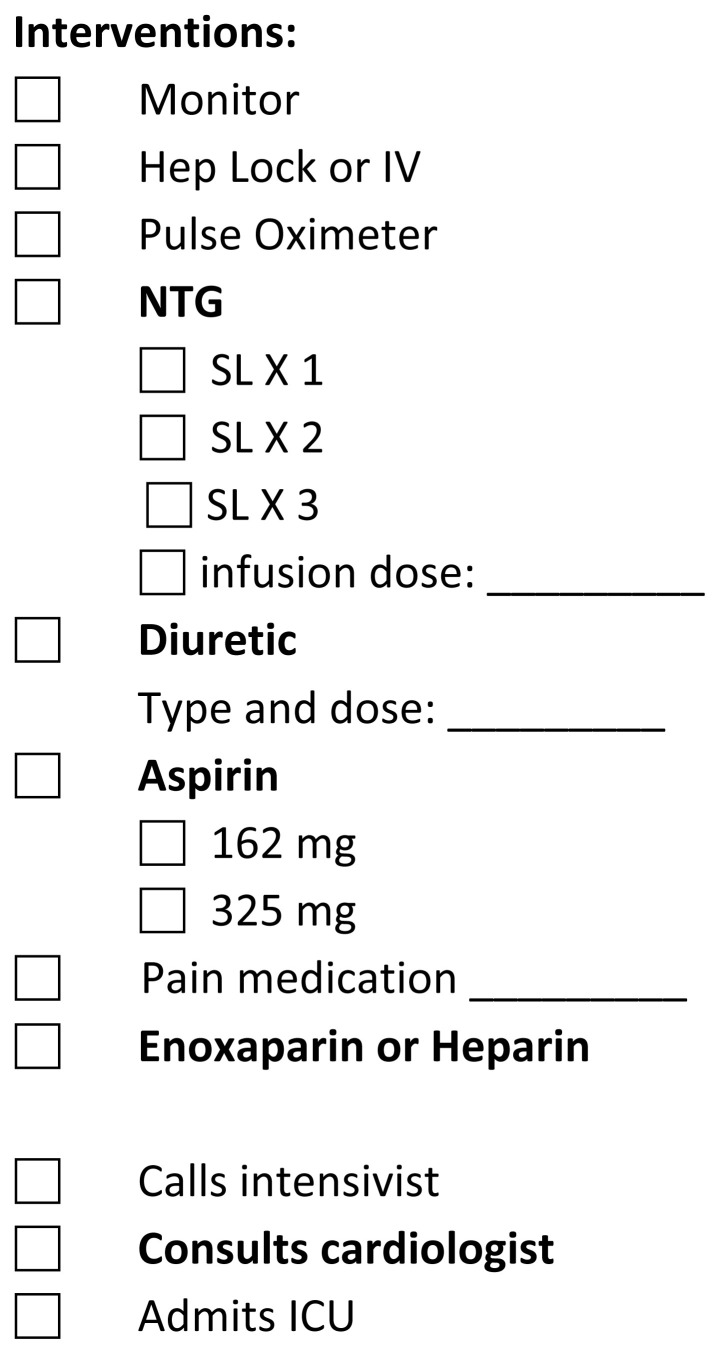
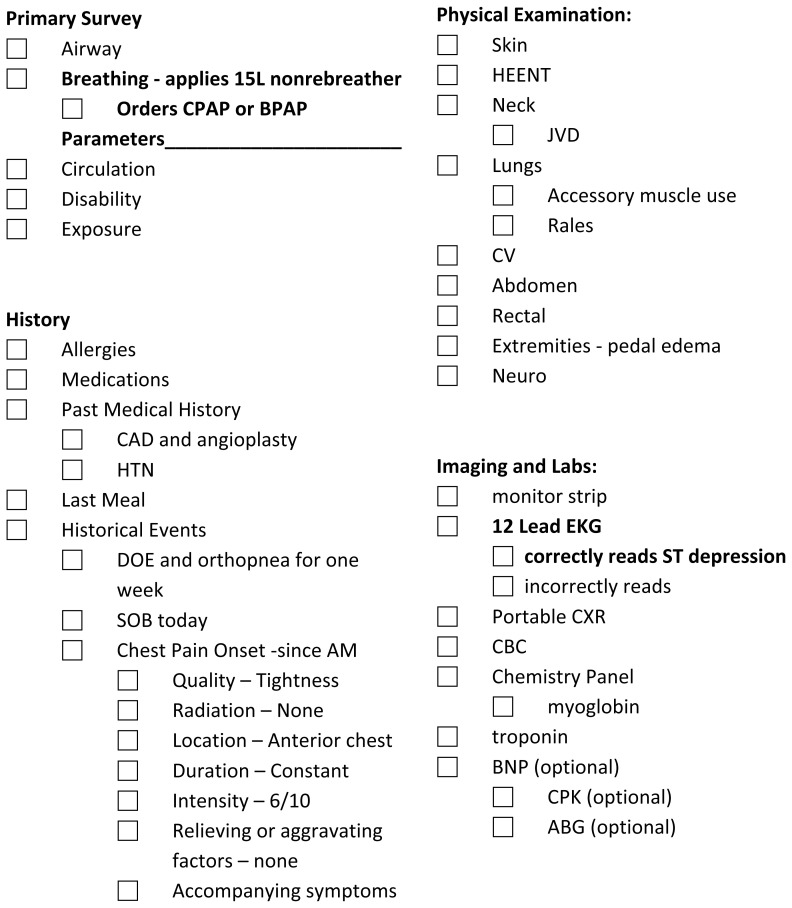
Discussion: Acute pulmonary edema and NSTEMI are common diagnoses that will be frequently encountered for most emergency physicians. This case highlights the need for early identification and aggressive management of the patient presenting with respiratory distress. The differential for respiratory distress is large, but most learners were able to quickly identify pulmonary edema based on the exam findings of jugular vein distention (JVD), rales, and lower extremity edema. Most learners quickly escalated to a non-rebreather mask and ultimately to BPAP (bilevel positive airway pressure) without requesting to intubate the patient. There was notable variation in the approach to administering nitrates, but most ordered an intravenous (IV) nitroglycerin (NTG) drip and requested pharmacy assistance in dosing. Diuretics were ordered by all the learners, but some were hesitant to start early because they felt the effect would be delayed. Some of the residents did not identify ischemic changes on the EKG at first glance but did request to review a second time when the troponin result was positive. All residents gave aspirin after noting the positive troponin, but not all were able to make a clear diagnosis of NSTEMI or consult cardiology. Although the case was relatively straightforward, residents enjoyed early diagnosis and aggressive management of the patient with impending respiratory failure. Many residents are asking for an ultrasound early in the workup of this patient presenting in respiratory distress. Although not a critical action in this case, it highlights the emphasis placed on ultrasonography in the current emergency medicine curriculum.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


