Jung Hyun Hong, Chan Woo Jung, Hoon Soo Kim, Yong Chan Bae
{"title":"下唇鳞状细胞癌切除的合适手术切缘。","authors":"Jung Hyun Hong, Chan Woo Jung, Hoon Soo Kim, Yong Chan Bae","doi":"10.1055/a-2095-6885","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b> Squamous cell carcinoma (SCC) is the most common malignancy on the lower lip. Surgical excision, the standard treatment for SCC, requires full-thickness excision. However, no consensus exists about the appropriate surgical margin. Therefore, we investigated the appropriate surgical margin and excision technique by analyzing 23 years of surgical experience with lower-lip SCC. <b>Methods</b> We reviewed 44 patients with lower-lip SCC who underwent surgery from November 1997 to October 2020. Frozen biopsy was performed with an appropriate margin on the left and right sides of the lesion, and the margin below the lesion was the skin above the sulcus boundary. If the frozen biopsy result was positive, an additional session was performed to secure a negative margin. Full-thickness excision was performed until the final negative margin. In each patient, the total number of sessions performed, final surgical margin, and recurrence were analyzed. <b>Results</b> Forty-one cases ended in the first session, 2 ended in the second session, and 1 ended in the third session. The final surgical margins (left and right; <i>n</i> = 88) were 5 mm (66%), 7 mm (9%), 8 mm (2.3%), 10 mm (20.4%), and 15 mm (2.3%). During an average follow-up of 67.4 months (range, 12-227 months), recurrence occurred in one patient. <b>Conclusion</b> The final surgical margin was 5 mm in 66% (58/88) of the cases, and 97.7% (86/88) were within 10 mm. Therefore, we set the first frozen biopsy margin to 5 mm, and we suggest that a 5-mm additional excision is appropriate when frozen biopsy results are positive.</p>","PeriodicalId":47543,"journal":{"name":"Archives of Plastic Surgery-APS","volume":"50 4","pages":"377-383"},"PeriodicalIF":1.3000,"publicationDate":"2023-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10411274/pdf/","citationCount":"0","resultStr":"{\"title\":\"Appropriate Surgical Margins for Excision of Squamous Cell Carcinoma of the Lower Lip.\",\"authors\":\"Jung Hyun Hong, Chan Woo Jung, Hoon Soo Kim, Yong Chan Bae\",\"doi\":\"10.1055/a-2095-6885\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background</b> Squamous cell carcinoma (SCC) is the most common malignancy on the lower lip. Surgical excision, the standard treatment for SCC, requires full-thickness excision. However, no consensus exists about the appropriate surgical margin. Therefore, we investigated the appropriate surgical margin and excision technique by analyzing 23 years of surgical experience with lower-lip SCC. <b>Methods</b> We reviewed 44 patients with lower-lip SCC who underwent surgery from November 1997 to October 2020. Frozen biopsy was performed with an appropriate margin on the left and right sides of the lesion, and the margin below the lesion was the skin above the sulcus boundary. If the frozen biopsy result was positive, an additional session was performed to secure a negative margin. Full-thickness excision was performed until the final negative margin. In each patient, the total number of sessions performed, final surgical margin, and recurrence were analyzed. <b>Results</b> Forty-one cases ended in the first session, 2 ended in the second session, and 1 ended in the third session. The final surgical margins (left and right; <i>n</i> = 88) were 5 mm (66%), 7 mm (9%), 8 mm (2.3%), 10 mm (20.4%), and 15 mm (2.3%). During an average follow-up of 67.4 months (range, 12-227 months), recurrence occurred in one patient. <b>Conclusion</b> The final surgical margin was 5 mm in 66% (58/88) of the cases, and 97.7% (86/88) were within 10 mm. Therefore, we set the first frozen biopsy margin to 5 mm, and we suggest that a 5-mm additional excision is appropriate when frozen biopsy results are positive.</p>\",\"PeriodicalId\":47543,\"journal\":{\"name\":\"Archives of Plastic Surgery-APS\",\"volume\":\"50 4\",\"pages\":\"377-383\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2023-08-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10411274/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archives of Plastic Surgery-APS\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2095-6885\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Plastic Surgery-APS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2095-6885","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Appropriate Surgical Margins for Excision of Squamous Cell Carcinoma of the Lower Lip.
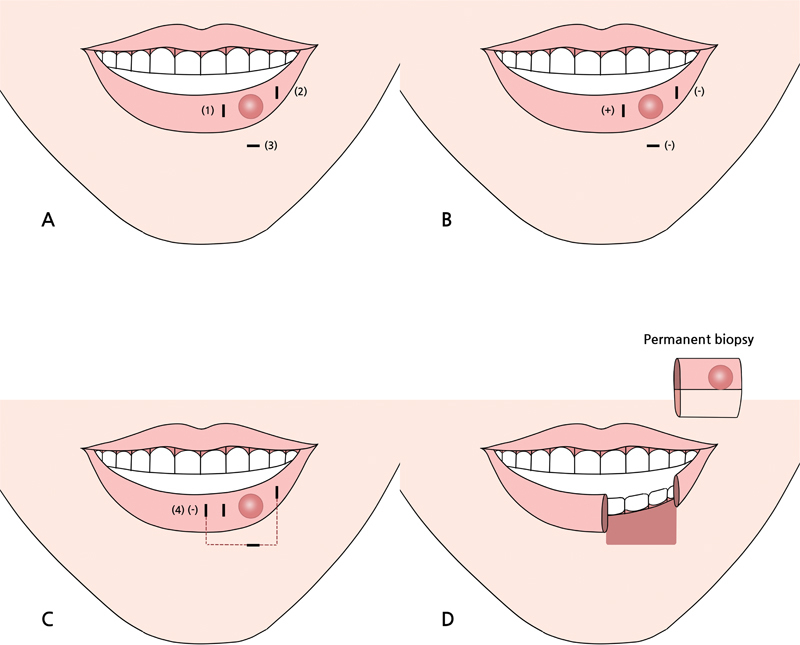
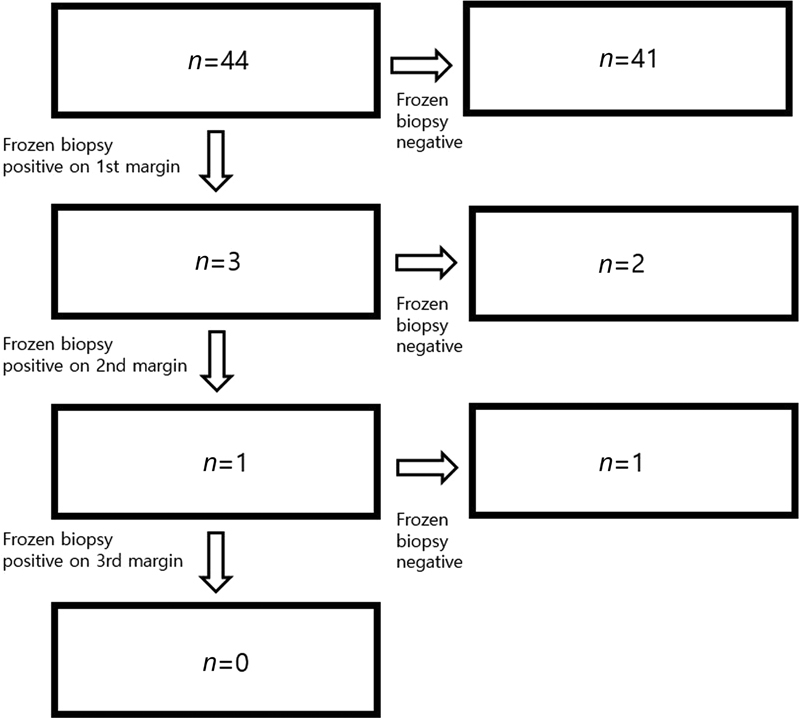
Background Squamous cell carcinoma (SCC) is the most common malignancy on the lower lip. Surgical excision, the standard treatment for SCC, requires full-thickness excision. However, no consensus exists about the appropriate surgical margin. Therefore, we investigated the appropriate surgical margin and excision technique by analyzing 23 years of surgical experience with lower-lip SCC. Methods We reviewed 44 patients with lower-lip SCC who underwent surgery from November 1997 to October 2020. Frozen biopsy was performed with an appropriate margin on the left and right sides of the lesion, and the margin below the lesion was the skin above the sulcus boundary. If the frozen biopsy result was positive, an additional session was performed to secure a negative margin. Full-thickness excision was performed until the final negative margin. In each patient, the total number of sessions performed, final surgical margin, and recurrence were analyzed. Results Forty-one cases ended in the first session, 2 ended in the second session, and 1 ended in the third session. The final surgical margins (left and right; n = 88) were 5 mm (66%), 7 mm (9%), 8 mm (2.3%), 10 mm (20.4%), and 15 mm (2.3%). During an average follow-up of 67.4 months (range, 12-227 months), recurrence occurred in one patient. Conclusion The final surgical margin was 5 mm in 66% (58/88) of the cases, and 97.7% (86/88) were within 10 mm. Therefore, we set the first frozen biopsy margin to 5 mm, and we suggest that a 5-mm additional excision is appropriate when frozen biopsy results are positive.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


