Sahith Reddy Thotamgari MD , Akhilesh Babbili MD , Prabandh Bucchanolla MD , Samarthkumar Thakkar MD , Harsh P. Patel MD , Maja B. Spaseski MD , Jonathan Graff-Radford MD , Alejandro A. Rabinstein MD , Zain Ul Abideen Asad MD, MS , Samuel J. Asirvatham MD , David R. Holmes Jr. MD , Abhishek Deshmukh MD , Christopher V. DeSimone MD, PhD
{"title":"房颤对非外伤性脑出血住院患者预后的影响","authors":"Sahith Reddy Thotamgari MD , Akhilesh Babbili MD , Prabandh Bucchanolla MD , Samarthkumar Thakkar MD , Harsh P. Patel MD , Maja B. Spaseski MD , Jonathan Graff-Radford MD , Alejandro A. Rabinstein MD , Zain Ul Abideen Asad MD, MS , Samuel J. Asirvatham MD , David R. Holmes Jr. MD , Abhishek Deshmukh MD , Christopher V. DeSimone MD, PhD","doi":"10.1016/j.mayocpiqo.2023.04.008","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>To assess the effect of atrial fibrillation (AF) on outcomes in hospitalizations for non-traumatic intracerebral hemorrhage (ICH).</p></div><div><h3>Patients and Methods</h3><p>We queried the National Inpatient Sample database between January 1, 2016, and December 31, 2019, to identify hospitalizations with an index diagnosis of non-traumatic ICH using ICD-10 code I61. The cohort was divided into patients with and without AF. Propensity score matching was used to balance the covariates between AF and non-AF groups. Logistic regression was used to analyze the association. All statistical analyses were performed using weighted values.</p></div><div><h3>Results</h3><p>Our cohort included 292,725 hospitalizations with a primary discharge diagnosis of non-traumatic ICH. From this group, 59,005 (20%) recorded a concurrent diagnosis of AF, and 46% of these patients with AF were taking anticoagulants. Patients with AF reported a higher Elixhauser comorbidity index (19.8±6.0 vs 16.6±6.4; <em>P</em><.001) before propensity matching. After propensity matching, the multivariate analysis reported that AF (aOR, 2.34; 95% CI, 2.26-2.42; <em>P</em><.001) and anticoagulation drug use (aOR, 1.32; 95% CI, 1.28-1.37; <em>P</em><.001) were independently associated with all-cause in-hospital mortality. Moreover, AF was significantly associated with respiratory failure requiring mechanical ventilation (odds ratio, 1.57; 95% CI, 1.52-1.62; <em>P</em><.001) and acute heart failure (odds ratio, 1.26; 95% CI, 1.19-1.33; <em>P</em><.001) compared with the absence of AF.</p></div><div><h3>Conclusion</h3><p>These data suggest that non-traumatic ICH hospitalizations with coexistent AF are associated with worse in-hospital outcomes such as higher mortality and acute heart failure.</p></div>","PeriodicalId":94132,"journal":{"name":"Mayo Clinic proceedings. Innovations, quality & outcomes","volume":"7 4","pages":"Pages 222-230"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/80/ce/main.PMC10250577.pdf","citationCount":"0","resultStr":"{\"title\":\"Impact of Atrial Fibrillation on Outcomes in Patients Hospitalized With Nontraumatic Intracerebral Hemorrhage\",\"authors\":\"Sahith Reddy Thotamgari MD , Akhilesh Babbili MD , Prabandh Bucchanolla MD , Samarthkumar Thakkar MD , Harsh P. Patel MD , Maja B. Spaseski MD , Jonathan Graff-Radford MD , Alejandro A. Rabinstein MD , Zain Ul Abideen Asad MD, MS , Samuel J. Asirvatham MD , David R. Holmes Jr. MD , Abhishek Deshmukh MD , Christopher V. DeSimone MD, PhD\",\"doi\":\"10.1016/j.mayocpiqo.2023.04.008\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><p>To assess the effect of atrial fibrillation (AF) on outcomes in hospitalizations for non-traumatic intracerebral hemorrhage (ICH).</p></div><div><h3>Patients and Methods</h3><p>We queried the National Inpatient Sample database between January 1, 2016, and December 31, 2019, to identify hospitalizations with an index diagnosis of non-traumatic ICH using ICD-10 code I61. The cohort was divided into patients with and without AF. Propensity score matching was used to balance the covariates between AF and non-AF groups. Logistic regression was used to analyze the association. All statistical analyses were performed using weighted values.</p></div><div><h3>Results</h3><p>Our cohort included 292,725 hospitalizations with a primary discharge diagnosis of non-traumatic ICH. From this group, 59,005 (20%) recorded a concurrent diagnosis of AF, and 46% of these patients with AF were taking anticoagulants. Patients with AF reported a higher Elixhauser comorbidity index (19.8±6.0 vs 16.6±6.4; <em>P</em><.001) before propensity matching. After propensity matching, the multivariate analysis reported that AF (aOR, 2.34; 95% CI, 2.26-2.42; <em>P</em><.001) and anticoagulation drug use (aOR, 1.32; 95% CI, 1.28-1.37; <em>P</em><.001) were independently associated with all-cause in-hospital mortality. Moreover, AF was significantly associated with respiratory failure requiring mechanical ventilation (odds ratio, 1.57; 95% CI, 1.52-1.62; <em>P</em><.001) and acute heart failure (odds ratio, 1.26; 95% CI, 1.19-1.33; <em>P</em><.001) compared with the absence of AF.</p></div><div><h3>Conclusion</h3><p>These data suggest that non-traumatic ICH hospitalizations with coexistent AF are associated with worse in-hospital outcomes such as higher mortality and acute heart failure.</p></div>\",\"PeriodicalId\":94132,\"journal\":{\"name\":\"Mayo Clinic proceedings. Innovations, quality & outcomes\",\"volume\":\"7 4\",\"pages\":\"Pages 222-230\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/80/ce/main.PMC10250577.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Mayo Clinic proceedings. Innovations, quality & outcomes\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2542454823000243\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mayo Clinic proceedings. Innovations, quality & outcomes","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2542454823000243","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的评估心房颤动(AF)对非创伤性脑出血(ICH)住院治疗结果的影响。患者和方法我们查询了2016年1月1日至2019年12月31日期间的全国住院患者样本数据库,以使用ICD-10代码I61确定非创伤性ICH指数诊断的住院患者。该队列被分为AF患者和非AF患者。倾向评分匹配用于平衡AF组和非AF组之间的协变量。采用Logistic回归分析其相关性。所有统计分析均使用加权值进行。结果我们的队列包括292725例以非创伤性脑出血为主要出院诊断的住院患者。这组患者中,59005人(20%)同时诊断为房颤,其中46%的房颤患者正在服用抗凝剂。AF患者在倾向匹配前报告了更高的Elixhauser合并症指数(19.8±6.0 vs 16.6±6.4;P<;.001)。倾向匹配后,多变量分析报告AF(aOR,2.34;95%CI,2.26-2.42;P<;.001)和抗凝药物使用(aOR、1.32;95%CI、1.28-1.37;P<:.001)与全因住院死亡率独立相关。此外与没有AF相比,AF与需要机械通气的呼吸衰竭(比值比,1.57;95%CI,1.52-1.62;P<;.001)和急性心力衰竭(比值比:1.26;95%CI:1.19-1.33;P<,.001)显著相关死亡率和急性心力衰竭。
Impact of Atrial Fibrillation on Outcomes in Patients Hospitalized With Nontraumatic Intracerebral Hemorrhage
Objective
To assess the effect of atrial fibrillation (AF) on outcomes in hospitalizations for non-traumatic intracerebral hemorrhage (ICH).
Patients and Methods
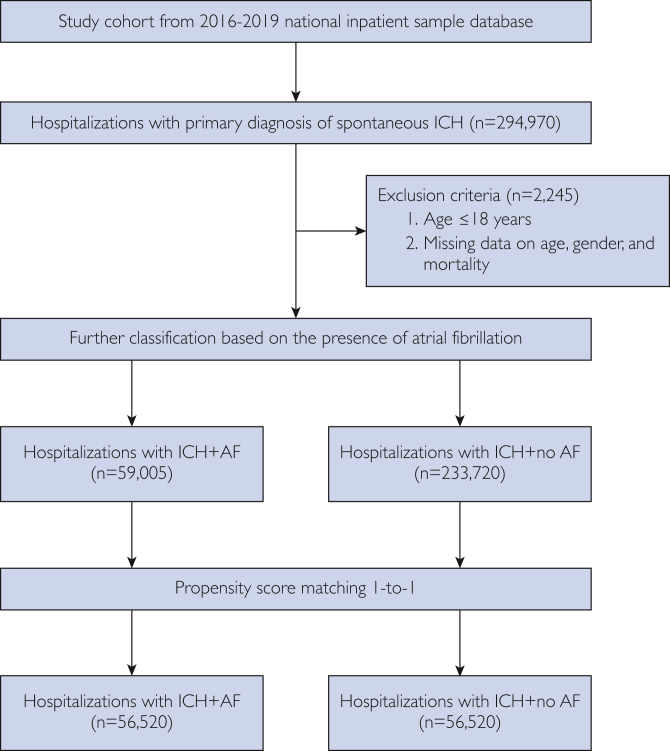
We queried the National Inpatient Sample database between January 1, 2016, and December 31, 2019, to identify hospitalizations with an index diagnosis of non-traumatic ICH using ICD-10 code I61. The cohort was divided into patients with and without AF. Propensity score matching was used to balance the covariates between AF and non-AF groups. Logistic regression was used to analyze the association. All statistical analyses were performed using weighted values.
Results
Our cohort included 292,725 hospitalizations with a primary discharge diagnosis of non-traumatic ICH. From this group, 59,005 (20%) recorded a concurrent diagnosis of AF, and 46% of these patients with AF were taking anticoagulants. Patients with AF reported a higher Elixhauser comorbidity index (19.8±6.0 vs 16.6±6.4; P<.001) before propensity matching. After propensity matching, the multivariate analysis reported that AF (aOR, 2.34; 95% CI, 2.26-2.42; P<.001) and anticoagulation drug use (aOR, 1.32; 95% CI, 1.28-1.37; P<.001) were independently associated with all-cause in-hospital mortality. Moreover, AF was significantly associated with respiratory failure requiring mechanical ventilation (odds ratio, 1.57; 95% CI, 1.52-1.62; P<.001) and acute heart failure (odds ratio, 1.26; 95% CI, 1.19-1.33; P<.001) compared with the absence of AF.
Conclusion
These data suggest that non-traumatic ICH hospitalizations with coexistent AF are associated with worse in-hospital outcomes such as higher mortality and acute heart failure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


