Afik D Snir, Martin K Ng, Geoff Strange, David Playford, Simon Stewart, David S Celermajer
{"title":"低梯度严重主动脉瓣狭窄患者卒中体积指数的预后意义:来自澳大利亚国家回声数据库。","authors":"Afik D Snir, Martin K Ng, Geoff Strange, David Playford, Simon Stewart, David S Celermajer","doi":"10.1007/s10554-023-02886-y","DOIUrl":null,"url":null,"abstract":"<p><p>Approximately 50% of patients with severe aortic stenosis (AS) in clinical practice present with 'low-gradient' haemodynamics. Stroke Volume Index (SVI) is a measure of left ventricular output, with 'normal-flow' considered as > 35 ml/m<sup>2</sup>. The association between SVI and prognosis in severe low-gradient AS (LGAS) in currently not well-understood. We analysed the National Echo Database of Australia (NEDA) and identified 109,990 patients with sufficiently comprehensive echocardiographic data, linked to survival information. We identified 1,699 with severe LGAS and preserved ejection fraction (EF) (≥ 50%) and 774 with severe LGAS and reduced EF. One- and three-year survival in each subgroup were assessed (follow-up of 74 ± 43 months), according to SVI thresholds. In patients with preserved EF the mortality \"threshold\" was at SVI < 30 ml/m<sup>2</sup>; 1- and 3-year survival was worse for those with SVI < 30 ml/m<sup>2</sup> relative to those with SVI > 35 ml/m<sup>2</sup> (HR 1.80, 95% CI 1.32-2.47 and HR 1.38, 95% CI 1.12-1.70), while survival was similar between those with SVI 30-35 ml/m<sup>2</sup> and SVI > 35 ml/m<sup>2</sup>. In patients with reduced EF the mortality \"threshold\" was 35 ml/m<sup>2</sup>; 1- and 3-year survival was worse for both those with SVI < 30 ml/m<sup>2</sup> and 30-35 ml/m<sup>2</sup> relative to those with SVI > 35 ml/m<sup>2</sup> (HR 1.98, 95% CI 1.27-3.09 and HR 1.41, 95% CI 1.05-1.93 for SVI < 30 ml/m<sup>2</sup> and HR 2.02, 95% CI 1.23-3.31 and HR 1.56, 95% CI 1.10-2.21 for SVI 30-35 ml/m<sup>2</sup>). The SVI prognostic threshold for medium-term mortality in severe LGAS patients is different for those with preserved LVEF (< 30 ml/m<sup>2</sup>) compared to those with reduced LVEF (< 35 ml/m<sup>2</sup>).</p>","PeriodicalId":50332,"journal":{"name":"International Journal of Cardiovascular Imaging","volume":" ","pages":"1719-1727"},"PeriodicalIF":1.5000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10520126/pdf/","citationCount":"0","resultStr":"{\"title\":\"The prognostic significance of stroke volume index in low gradient severe aortic stenosis: from the national echo database of Australia.\",\"authors\":\"Afik D Snir, Martin K Ng, Geoff Strange, David Playford, Simon Stewart, David S Celermajer\",\"doi\":\"10.1007/s10554-023-02886-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Approximately 50% of patients with severe aortic stenosis (AS) in clinical practice present with 'low-gradient' haemodynamics. Stroke Volume Index (SVI) is a measure of left ventricular output, with 'normal-flow' considered as > 35 ml/m<sup>2</sup>. The association between SVI and prognosis in severe low-gradient AS (LGAS) in currently not well-understood. We analysed the National Echo Database of Australia (NEDA) and identified 109,990 patients with sufficiently comprehensive echocardiographic data, linked to survival information. We identified 1,699 with severe LGAS and preserved ejection fraction (EF) (≥ 50%) and 774 with severe LGAS and reduced EF. One- and three-year survival in each subgroup were assessed (follow-up of 74 ± 43 months), according to SVI thresholds. In patients with preserved EF the mortality \\\"threshold\\\" was at SVI < 30 ml/m<sup>2</sup>; 1- and 3-year survival was worse for those with SVI < 30 ml/m<sup>2</sup> relative to those with SVI > 35 ml/m<sup>2</sup> (HR 1.80, 95% CI 1.32-2.47 and HR 1.38, 95% CI 1.12-1.70), while survival was similar between those with SVI 30-35 ml/m<sup>2</sup> and SVI > 35 ml/m<sup>2</sup>. In patients with reduced EF the mortality \\\"threshold\\\" was 35 ml/m<sup>2</sup>; 1- and 3-year survival was worse for both those with SVI < 30 ml/m<sup>2</sup> and 30-35 ml/m<sup>2</sup> relative to those with SVI > 35 ml/m<sup>2</sup> (HR 1.98, 95% CI 1.27-3.09 and HR 1.41, 95% CI 1.05-1.93 for SVI < 30 ml/m<sup>2</sup> and HR 2.02, 95% CI 1.23-3.31 and HR 1.56, 95% CI 1.10-2.21 for SVI 30-35 ml/m<sup>2</sup>). The SVI prognostic threshold for medium-term mortality in severe LGAS patients is different for those with preserved LVEF (< 30 ml/m<sup>2</sup>) compared to those with reduced LVEF (< 35 ml/m<sup>2</sup>).</p>\",\"PeriodicalId\":50332,\"journal\":{\"name\":\"International Journal of Cardiovascular Imaging\",\"volume\":\" \",\"pages\":\"1719-1727\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10520126/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Cardiovascular Imaging\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10554-023-02886-y\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/6/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Cardiovascular Imaging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10554-023-02886-y","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/10 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
The prognostic significance of stroke volume index in low gradient severe aortic stenosis: from the national echo database of Australia.
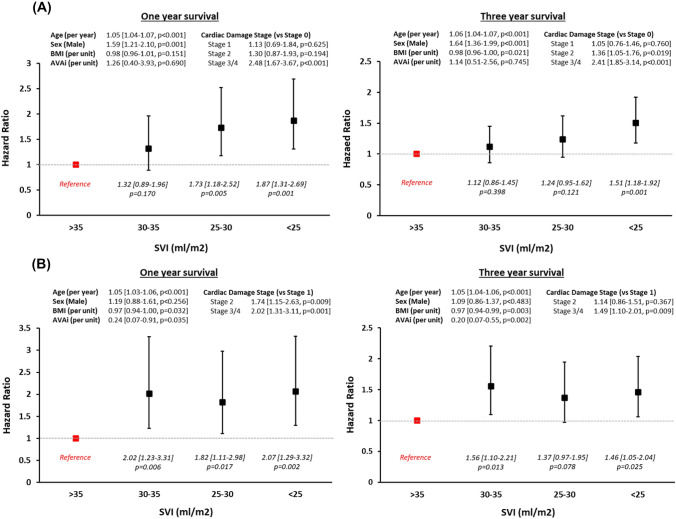
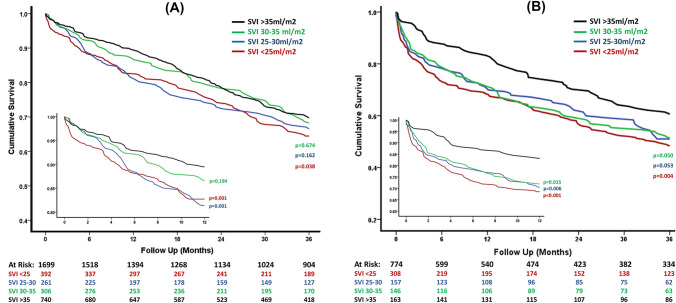
Approximately 50% of patients with severe aortic stenosis (AS) in clinical practice present with 'low-gradient' haemodynamics. Stroke Volume Index (SVI) is a measure of left ventricular output, with 'normal-flow' considered as > 35 ml/m2. The association between SVI and prognosis in severe low-gradient AS (LGAS) in currently not well-understood. We analysed the National Echo Database of Australia (NEDA) and identified 109,990 patients with sufficiently comprehensive echocardiographic data, linked to survival information. We identified 1,699 with severe LGAS and preserved ejection fraction (EF) (≥ 50%) and 774 with severe LGAS and reduced EF. One- and three-year survival in each subgroup were assessed (follow-up of 74 ± 43 months), according to SVI thresholds. In patients with preserved EF the mortality "threshold" was at SVI < 30 ml/m2; 1- and 3-year survival was worse for those with SVI < 30 ml/m2 relative to those with SVI > 35 ml/m2 (HR 1.80, 95% CI 1.32-2.47 and HR 1.38, 95% CI 1.12-1.70), while survival was similar between those with SVI 30-35 ml/m2 and SVI > 35 ml/m2. In patients with reduced EF the mortality "threshold" was 35 ml/m2; 1- and 3-year survival was worse for both those with SVI < 30 ml/m2 and 30-35 ml/m2 relative to those with SVI > 35 ml/m2 (HR 1.98, 95% CI 1.27-3.09 and HR 1.41, 95% CI 1.05-1.93 for SVI < 30 ml/m2 and HR 2.02, 95% CI 1.23-3.31 and HR 1.56, 95% CI 1.10-2.21 for SVI 30-35 ml/m2). The SVI prognostic threshold for medium-term mortality in severe LGAS patients is different for those with preserved LVEF (< 30 ml/m2) compared to those with reduced LVEF (< 35 ml/m2).
期刊介绍:
The International Journal of Cardiovascular Imaging publishes technical and clinical communications (original articles, review articles and editorial comments) associated with cardiovascular diseases. The technical communications include the research, development and evaluation of novel imaging methods in the various imaging domains. These domains include magnetic resonance imaging, computed tomography, X-ray imaging, intravascular imaging, and applications in nuclear cardiology and echocardiography, and any combination of these techniques. Of particular interest are topics in medical image processing and image-guided interventions. Clinical applications of such imaging techniques include improved diagnostic approaches, treatment , prognosis and follow-up of cardiovascular patients. Topics include: multi-center or larger individual studies dealing with risk stratification and imaging utilization, applications for better characterization of cardiovascular diseases, and assessment of the efficacy of new drugs and interventional devices.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


