Ann Livingstone, Kirsten Howard, Alexander M Menzies, Georgina V Long, Martin R Stockler, Rachael L Morton
{"title":"已切除 III 期黑色素瘤成人对辅助免疫疗法的偏好--离散选择实验。","authors":"Ann Livingstone, Kirsten Howard, Alexander M Menzies, Georgina V Long, Martin R Stockler, Rachael L Morton","doi":"10.1007/s40271-023-00635-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This study aimed to quantify adult preferences for adjuvant immunotherapy for resected melanoma and the influence of varying levels of key attributes and baseline characteristics.</p><p><strong>Methods: </strong>A D-efficient design generated 12 choice tasks for two alternative treatments, adjuvant immunotherapy or no adjuvant immunotherapy. Recruitment to the online discrete choice experiment (DCE) occurred via survey dissemination by eight Australian melanoma consumer and professional groups, targeting adults with resected stage III melanoma, considering or having received adjuvant immunotherapy. The DCE included six attributes with two to three levels each, including 3-year risk of recurrence, mild, permanent and fatal adverse events (AEs), drug regimen and annual out-of-pocket costs. A mixed multinomial logit model was used to estimate preferences and calculate marginal rates of substitution and marginal willingness to pay (mWTP).</p><p><strong>Results: </strong>The DCE was completed by 116 respondents, who chose adjuvant immunotherapy over no adjuvant immunotherapy in 70% of choice tasks. Respondents preferred adjuvant immunotherapy when associated with reduced: probabilities of recurrence, permanent and fatal AEs, and out-of-pocket costs. mWTP for an absolute reduction of 1% in 3-year risk of recurrence was less for respondents with lower rather than higher incomes, AU$794 (US$527) and AU$2190 (US$1454) per year. Respondents accepted an additional 4% chance of a permanent AE to reduce their absolute risk of 3-year recurrence by 1%. Respondents were willing to accept an extra 2% chance of 3-year recurrence to lower their chance of a fatal AE by 1%.</p><p><strong>Conclusions: </strong>Almost three-quarters of respondents chose adjuvant immunotherapy over no adjuvant immunotherapy, preferring treatment that improved efficacy and safety. Findings may inform decisions about access to adjuvant immunotherapy following surgery for melanoma.</p>","PeriodicalId":51271,"journal":{"name":"Patient-Patient Centered Outcomes Research","volume":"16 5","pages":"497-513"},"PeriodicalIF":3.1000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/51/ca/40271_2023_Article_635.PMC10409831.pdf","citationCount":"1","resultStr":"{\"title\":\"Preferences for Adjuvant Immunotherapy in Adults with Resected Stage III Melanoma-A Discrete Choice Experiment.\",\"authors\":\"Ann Livingstone, Kirsten Howard, Alexander M Menzies, Georgina V Long, Martin R Stockler, Rachael L Morton\",\"doi\":\"10.1007/s40271-023-00635-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>This study aimed to quantify adult preferences for adjuvant immunotherapy for resected melanoma and the influence of varying levels of key attributes and baseline characteristics.</p><p><strong>Methods: </strong>A D-efficient design generated 12 choice tasks for two alternative treatments, adjuvant immunotherapy or no adjuvant immunotherapy. Recruitment to the online discrete choice experiment (DCE) occurred via survey dissemination by eight Australian melanoma consumer and professional groups, targeting adults with resected stage III melanoma, considering or having received adjuvant immunotherapy. The DCE included six attributes with two to three levels each, including 3-year risk of recurrence, mild, permanent and fatal adverse events (AEs), drug regimen and annual out-of-pocket costs. A mixed multinomial logit model was used to estimate preferences and calculate marginal rates of substitution and marginal willingness to pay (mWTP).</p><p><strong>Results: </strong>The DCE was completed by 116 respondents, who chose adjuvant immunotherapy over no adjuvant immunotherapy in 70% of choice tasks. Respondents preferred adjuvant immunotherapy when associated with reduced: probabilities of recurrence, permanent and fatal AEs, and out-of-pocket costs. mWTP for an absolute reduction of 1% in 3-year risk of recurrence was less for respondents with lower rather than higher incomes, AU$794 (US$527) and AU$2190 (US$1454) per year. Respondents accepted an additional 4% chance of a permanent AE to reduce their absolute risk of 3-year recurrence by 1%. Respondents were willing to accept an extra 2% chance of 3-year recurrence to lower their chance of a fatal AE by 1%.</p><p><strong>Conclusions: </strong>Almost three-quarters of respondents chose adjuvant immunotherapy over no adjuvant immunotherapy, preferring treatment that improved efficacy and safety. Findings may inform decisions about access to adjuvant immunotherapy following surgery for melanoma.</p>\",\"PeriodicalId\":51271,\"journal\":{\"name\":\"Patient-Patient Centered Outcomes Research\",\"volume\":\"16 5\",\"pages\":\"497-513\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/51/ca/40271_2023_Article_635.PMC10409831.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Patient-Patient Centered Outcomes Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40271-023-00635-w\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/6/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Patient-Patient Centered Outcomes Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40271-023-00635-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/23 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Preferences for Adjuvant Immunotherapy in Adults with Resected Stage III Melanoma-A Discrete Choice Experiment.
Objectives: This study aimed to quantify adult preferences for adjuvant immunotherapy for resected melanoma and the influence of varying levels of key attributes and baseline characteristics.
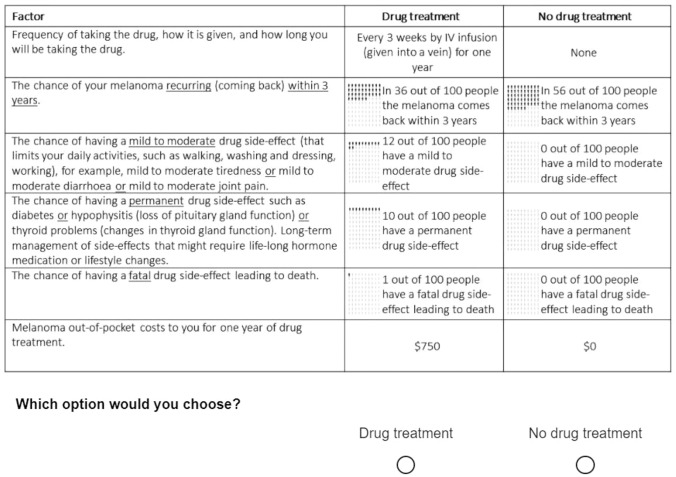
Methods: A D-efficient design generated 12 choice tasks for two alternative treatments, adjuvant immunotherapy or no adjuvant immunotherapy. Recruitment to the online discrete choice experiment (DCE) occurred via survey dissemination by eight Australian melanoma consumer and professional groups, targeting adults with resected stage III melanoma, considering or having received adjuvant immunotherapy. The DCE included six attributes with two to three levels each, including 3-year risk of recurrence, mild, permanent and fatal adverse events (AEs), drug regimen and annual out-of-pocket costs. A mixed multinomial logit model was used to estimate preferences and calculate marginal rates of substitution and marginal willingness to pay (mWTP).
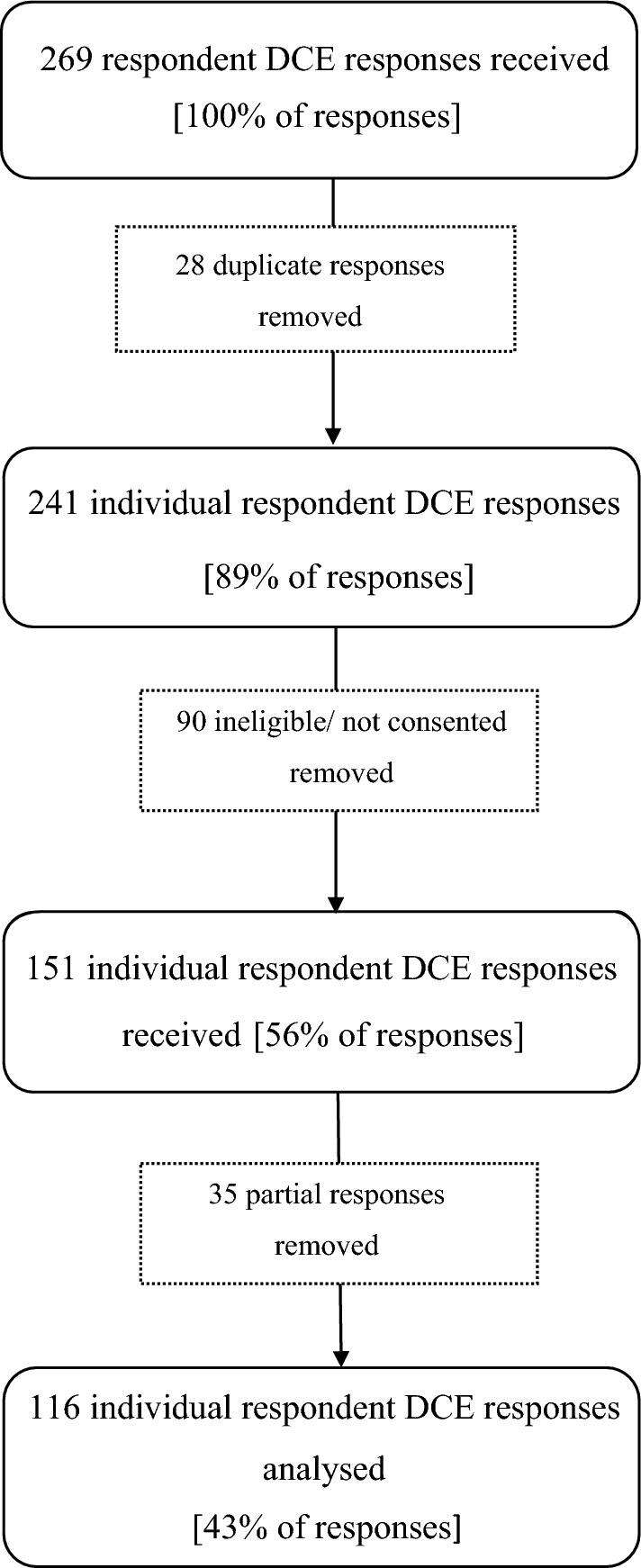
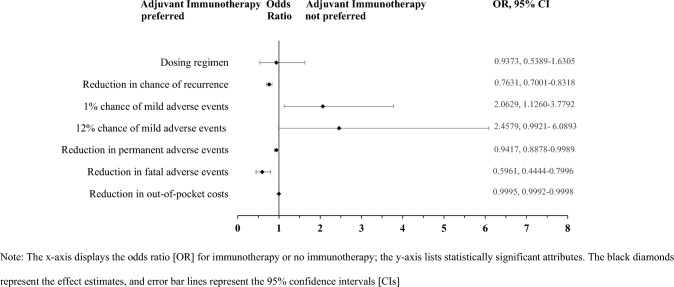
Results: The DCE was completed by 116 respondents, who chose adjuvant immunotherapy over no adjuvant immunotherapy in 70% of choice tasks. Respondents preferred adjuvant immunotherapy when associated with reduced: probabilities of recurrence, permanent and fatal AEs, and out-of-pocket costs. mWTP for an absolute reduction of 1% in 3-year risk of recurrence was less for respondents with lower rather than higher incomes, AU$794 (US$527) and AU$2190 (US$1454) per year. Respondents accepted an additional 4% chance of a permanent AE to reduce their absolute risk of 3-year recurrence by 1%. Respondents were willing to accept an extra 2% chance of 3-year recurrence to lower their chance of a fatal AE by 1%.
Conclusions: Almost three-quarters of respondents chose adjuvant immunotherapy over no adjuvant immunotherapy, preferring treatment that improved efficacy and safety. Findings may inform decisions about access to adjuvant immunotherapy following surgery for melanoma.
期刊介绍:
The Patient provides a venue for scientifically rigorous, timely, and relevant research to promote the development, evaluation and implementation of therapies, technologies, and innovations that will enhance the patient experience. It is an international forum for research that advances and/or applies qualitative or quantitative methods to promote the generation, synthesis, or interpretation of evidence.
The journal has specific interest in receiving original research, reviews and commentaries related to qualitative and mixed methods research, stated-preference methods, patient reported outcomes, and shared decision making.
Advances in regulatory science, patient-focused drug development, patient-centered benefit-risk and health technology assessment will also be considered.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in The Patient may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.
All manuscripts are subject to peer review by international experts.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


