Jaehyung Ha, Chan Joo Lee, Jaewon Oh, Sungha Park, Sang-Hak Lee, Seok-Min Kang
{"title":"射血分数减低型心力衰竭患者治疗期间非卧床中心血压与左心室逆重塑之间的关系","authors":"Jaehyung Ha, Chan Joo Lee, Jaewon Oh, Sungha Park, Sang-Hak Lee, Seok-Min Kang","doi":"10.36628/ijhf.2023.0004","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Compared to office blood pressure (OBP), central blood pressure (CBP) and ambulatory blood pressure (BP) are known to be better markers for predicting cardiovascular events. We evaluated the association between left ventricular reverse remodeling (LVRR) and ambulatory CBP in heart failure with reduced ejection fraction (HFrEF).</p><p><strong>Methods: </strong>This study retrospectively analyzed 93 patients who performed ambulatory CBP and brachial BP (BBP) monitoring from 2018 to 2020 within 1 year after diagnosis of HFrEF at a single tertiary center. We analyzed the association between on-treatment ambulatory BPs and LVRR on follow-up echocardiography.</p><p><strong>Results: </strong>The mean age of participants was 59 years; 65.6% were men; mean LVEF was 29%. Ambulatory BP and follow-up echocardiography were done at 143 days (interquartile range [IQR], 64-267) and 454 days (IQR, 281-600) after diagnosis of HF, respectively. Baseline OBP was not different between 2 groups, but ambulatory systolic CBP was significantly higher in the LVRR group than the non-LVRR group (p=0.005). Systolic OBP (odds ratio [OR], 1.029; confidence interval [CI], 1.004-1.055; p=0.026), 24-hour ambulatory systolic CBP (OR, 1.048; CI, 1.015-1.082; p=0.004), and 24-hour ambulatory systolic BBP (OR, 1.049; CI,1.017-1.082; p=0.003) were associated with LVRR. Compared to ambulatory systolic CBP of 110-119 mmHg, 90-99 mmHg showed lower OR for LVRR.</p><p><strong>Conclusions: </strong>Low on-treatment ambulatory systolic CBP was closely related to a lower likelihood of LVRR in HFrEF than the normal range. Ambulatory CBP measured during treatment of patients with HFrEF appears to be useful in predicting outcomes.</p>","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"5 3","pages":"150-158"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ec/4a/ijhf-5-150.PMC10406559.pdf","citationCount":"0","resultStr":"{\"title\":\"The Association Between On-treatment Ambulatory Central Blood Pressure and Left Ventricular Reverse Remodeling in Heart Failure With Reduced Ejection Fraction.\",\"authors\":\"Jaehyung Ha, Chan Joo Lee, Jaewon Oh, Sungha Park, Sang-Hak Lee, Seok-Min Kang\",\"doi\":\"10.36628/ijhf.2023.0004\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Compared to office blood pressure (OBP), central blood pressure (CBP) and ambulatory blood pressure (BP) are known to be better markers for predicting cardiovascular events. We evaluated the association between left ventricular reverse remodeling (LVRR) and ambulatory CBP in heart failure with reduced ejection fraction (HFrEF).</p><p><strong>Methods: </strong>This study retrospectively analyzed 93 patients who performed ambulatory CBP and brachial BP (BBP) monitoring from 2018 to 2020 within 1 year after diagnosis of HFrEF at a single tertiary center. We analyzed the association between on-treatment ambulatory BPs and LVRR on follow-up echocardiography.</p><p><strong>Results: </strong>The mean age of participants was 59 years; 65.6% were men; mean LVEF was 29%. Ambulatory BP and follow-up echocardiography were done at 143 days (interquartile range [IQR], 64-267) and 454 days (IQR, 281-600) after diagnosis of HF, respectively. Baseline OBP was not different between 2 groups, but ambulatory systolic CBP was significantly higher in the LVRR group than the non-LVRR group (p=0.005). Systolic OBP (odds ratio [OR], 1.029; confidence interval [CI], 1.004-1.055; p=0.026), 24-hour ambulatory systolic CBP (OR, 1.048; CI, 1.015-1.082; p=0.004), and 24-hour ambulatory systolic BBP (OR, 1.049; CI,1.017-1.082; p=0.003) were associated with LVRR. Compared to ambulatory systolic CBP of 110-119 mmHg, 90-99 mmHg showed lower OR for LVRR.</p><p><strong>Conclusions: </strong>Low on-treatment ambulatory systolic CBP was closely related to a lower likelihood of LVRR in HFrEF than the normal range. Ambulatory CBP measured during treatment of patients with HFrEF appears to be useful in predicting outcomes.</p>\",\"PeriodicalId\":14058,\"journal\":{\"name\":\"International Journal of Heart Failure\",\"volume\":\"5 3\",\"pages\":\"150-158\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ec/4a/ijhf-5-150.PMC10406559.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Heart Failure\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36628/ijhf.2023.0004\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2023.0004","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
The Association Between On-treatment Ambulatory Central Blood Pressure and Left Ventricular Reverse Remodeling in Heart Failure With Reduced Ejection Fraction.
Background and objectives: Compared to office blood pressure (OBP), central blood pressure (CBP) and ambulatory blood pressure (BP) are known to be better markers for predicting cardiovascular events. We evaluated the association between left ventricular reverse remodeling (LVRR) and ambulatory CBP in heart failure with reduced ejection fraction (HFrEF).
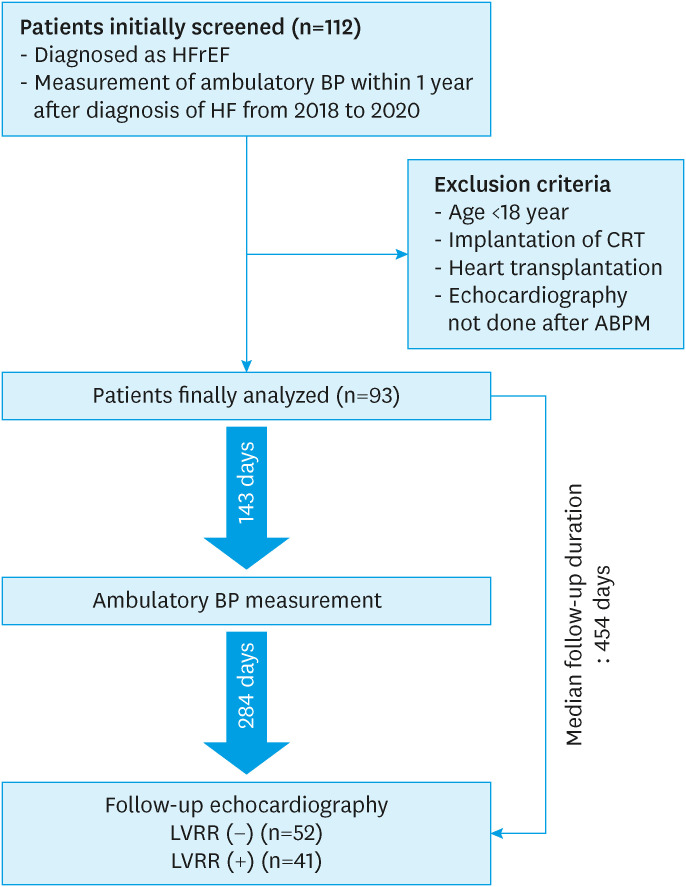
Methods: This study retrospectively analyzed 93 patients who performed ambulatory CBP and brachial BP (BBP) monitoring from 2018 to 2020 within 1 year after diagnosis of HFrEF at a single tertiary center. We analyzed the association between on-treatment ambulatory BPs and LVRR on follow-up echocardiography.
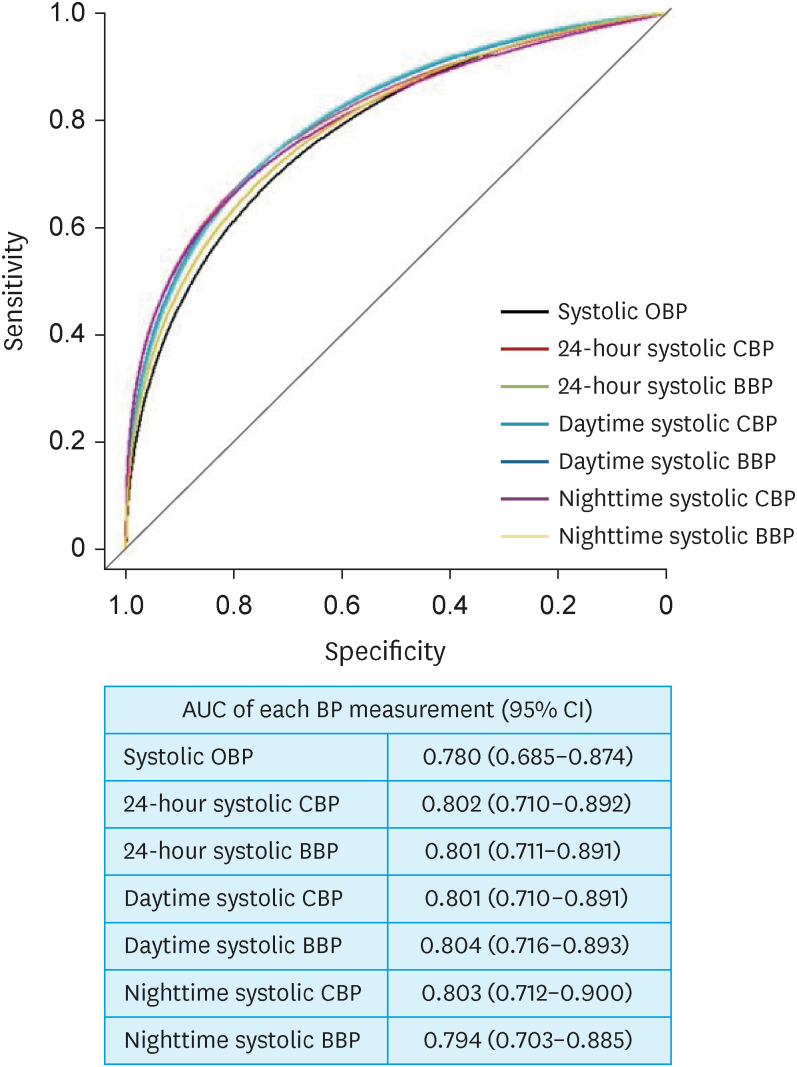
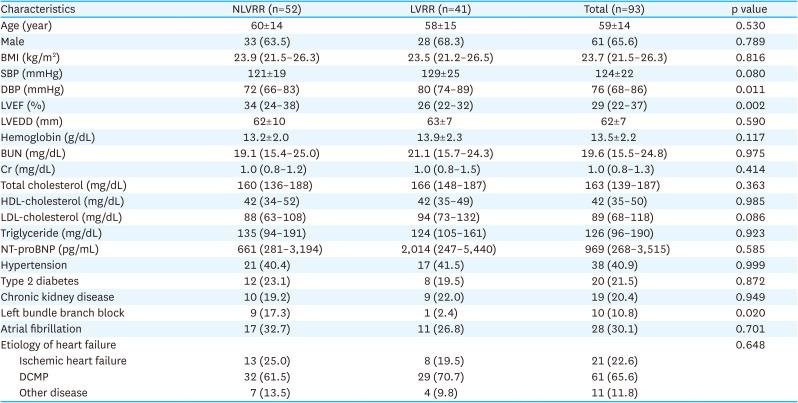
Results: The mean age of participants was 59 years; 65.6% were men; mean LVEF was 29%. Ambulatory BP and follow-up echocardiography were done at 143 days (interquartile range [IQR], 64-267) and 454 days (IQR, 281-600) after diagnosis of HF, respectively. Baseline OBP was not different between 2 groups, but ambulatory systolic CBP was significantly higher in the LVRR group than the non-LVRR group (p=0.005). Systolic OBP (odds ratio [OR], 1.029; confidence interval [CI], 1.004-1.055; p=0.026), 24-hour ambulatory systolic CBP (OR, 1.048; CI, 1.015-1.082; p=0.004), and 24-hour ambulatory systolic BBP (OR, 1.049; CI,1.017-1.082; p=0.003) were associated with LVRR. Compared to ambulatory systolic CBP of 110-119 mmHg, 90-99 mmHg showed lower OR for LVRR.
Conclusions: Low on-treatment ambulatory systolic CBP was closely related to a lower likelihood of LVRR in HFrEF than the normal range. Ambulatory CBP measured during treatment of patients with HFrEF appears to be useful in predicting outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


