Katalin Gaspar, Ramsis Croes, Misja Mikkers, Xander Koolman
{"title":"住院时间与经济激励:来自荷兰康复中心的证据。","authors":"Katalin Gaspar, Ramsis Croes, Misja Mikkers, Xander Koolman","doi":"10.1007/s10198-023-01615-5","DOIUrl":null,"url":null,"abstract":"<p><p>Non-linear reimbursement contracts in healthcare have been increasingly used to quantify providers' responses to financial incentives. In the present research, we utilize a large one-off increase in the reimbursement of rehabilitation care to assess to what extent providers are willing to modify their treating behavior to maximize profits. In order to disincentivize the use of short inpatient stays for rehabilitation care, Dutch policy-makers have instated a two-part stepwise tariff-schedule. A lower tariff-schedule is applied for short hospital stays (≤ 14 days), while a higher tariff-schedule is utilized for longer treatments. Switching from one schedule to the other at day 15 of inpatient care leads to a sudden and large increase in tariffs. We show that, for most care-types, patients are seldom treated in an inpatient setting for less than 15 days, while the majority of patients are discharged after the threshold. Therefore, we conclude that the financial incentive at day 15 leads to considerable distortions in treatment. However, instead of discharging all patients at the threshold point where marginal tariffs are maximized, providers tend to continue treatment indicating altruistic behavior. As healthcare payment systems move away from piecewise reimbursement (e.g., fee-for-service arrangements), and services are increasingly 'lumped' together into e.g., DRGs and bundled payments, the likelihood of such discontinuities in tariff-schedules radically increases. Our research illustrates how such discontinuities in reimbursements can lead to distortions in the amount of healthcare provided contributing to the debate on optimal healthcare contracting design.</p>","PeriodicalId":51416,"journal":{"name":"European Journal of Health Economics","volume":" ","pages":"731-741"},"PeriodicalIF":3.1000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11192693/pdf/","citationCount":"0","resultStr":"{\"title\":\"Length of hospital stays and financial incentives: evidence from Dutch rehabilitation centers.\",\"authors\":\"Katalin Gaspar, Ramsis Croes, Misja Mikkers, Xander Koolman\",\"doi\":\"10.1007/s10198-023-01615-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Non-linear reimbursement contracts in healthcare have been increasingly used to quantify providers' responses to financial incentives. In the present research, we utilize a large one-off increase in the reimbursement of rehabilitation care to assess to what extent providers are willing to modify their treating behavior to maximize profits. In order to disincentivize the use of short inpatient stays for rehabilitation care, Dutch policy-makers have instated a two-part stepwise tariff-schedule. A lower tariff-schedule is applied for short hospital stays (≤ 14 days), while a higher tariff-schedule is utilized for longer treatments. Switching from one schedule to the other at day 15 of inpatient care leads to a sudden and large increase in tariffs. We show that, for most care-types, patients are seldom treated in an inpatient setting for less than 15 days, while the majority of patients are discharged after the threshold. Therefore, we conclude that the financial incentive at day 15 leads to considerable distortions in treatment. However, instead of discharging all patients at the threshold point where marginal tariffs are maximized, providers tend to continue treatment indicating altruistic behavior. As healthcare payment systems move away from piecewise reimbursement (e.g., fee-for-service arrangements), and services are increasingly 'lumped' together into e.g., DRGs and bundled payments, the likelihood of such discontinuities in tariff-schedules radically increases. Our research illustrates how such discontinuities in reimbursements can lead to distortions in the amount of healthcare provided contributing to the debate on optimal healthcare contracting design.</p>\",\"PeriodicalId\":51416,\"journal\":{\"name\":\"European Journal of Health Economics\",\"volume\":\" \",\"pages\":\"731-741\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11192693/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Health Economics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10198-023-01615-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/8/9 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Health Economics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10198-023-01615-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/9 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
Length of hospital stays and financial incentives: evidence from Dutch rehabilitation centers.
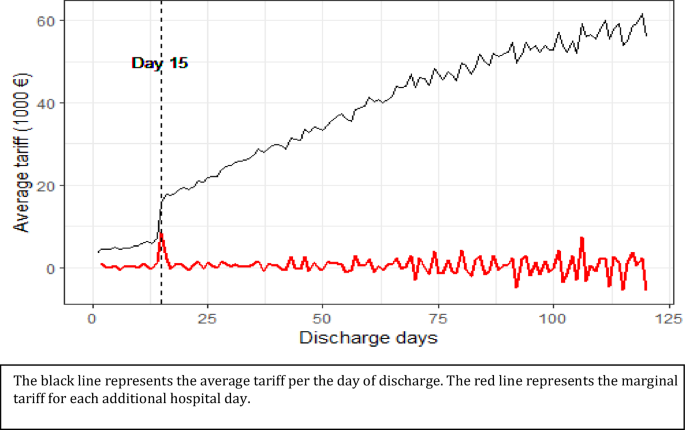
Non-linear reimbursement contracts in healthcare have been increasingly used to quantify providers' responses to financial incentives. In the present research, we utilize a large one-off increase in the reimbursement of rehabilitation care to assess to what extent providers are willing to modify their treating behavior to maximize profits. In order to disincentivize the use of short inpatient stays for rehabilitation care, Dutch policy-makers have instated a two-part stepwise tariff-schedule. A lower tariff-schedule is applied for short hospital stays (≤ 14 days), while a higher tariff-schedule is utilized for longer treatments. Switching from one schedule to the other at day 15 of inpatient care leads to a sudden and large increase in tariffs. We show that, for most care-types, patients are seldom treated in an inpatient setting for less than 15 days, while the majority of patients are discharged after the threshold. Therefore, we conclude that the financial incentive at day 15 leads to considerable distortions in treatment. However, instead of discharging all patients at the threshold point where marginal tariffs are maximized, providers tend to continue treatment indicating altruistic behavior. As healthcare payment systems move away from piecewise reimbursement (e.g., fee-for-service arrangements), and services are increasingly 'lumped' together into e.g., DRGs and bundled payments, the likelihood of such discontinuities in tariff-schedules radically increases. Our research illustrates how such discontinuities in reimbursements can lead to distortions in the amount of healthcare provided contributing to the debate on optimal healthcare contracting design.
期刊介绍:
The European Journal of Health Economics is a journal of Health Economics and associated disciplines. The growing demand for health economics and the introduction of new guidelines in various European countries were the motivation to generate a highly scientific and at the same time practice oriented journal considering the requirements of various health care systems in Europe. The international scientific board of opinion leaders guarantees high-quality, peer-reviewed publications as well as articles for pragmatic approaches in the field of health economics. We intend to cover all aspects of health economics:
• Basics of health economic approaches and methods
• Pharmacoeconomics
• Health Care Systems
• Pricing and Reimbursement Systems
• Quality-of-Life-Studies The editors reserve the right to reject manuscripts that do not comply with the above-mentioned requirements. The author will be held responsible for false statements or for failure to fulfill the above-mentioned requirements.
Officially cited as: Eur J Health Econ

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


