Jenny Lu-Song, Jeffrey A Bakal, Sarah Younus, Onofre Moran-Mendoza, Ingrid Harle, Michelle Morales, Naomi Rippon, Shaney L Barratt, Huzaifa Adamali, Meena Kalluri
{"title":"综合姑息治疗对特发性肺纤维化患者生存期的影响:多中心回顾性比较","authors":"Jenny Lu-Song, Jeffrey A Bakal, Sarah Younus, Onofre Moran-Mendoza, Ingrid Harle, Michelle Morales, Naomi Rippon, Shaney L Barratt, Huzaifa Adamali, Meena Kalluri","doi":"10.1177/10499091231194722","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Early and integrated palliative care is recommended for patients with idiopathic pulmonary fibrosis. Unfortunately, palliative care delivery remains poor due to various barriers in practice. This study describes various palliative care delivery models in a real-world cohort of patients with idiopathic pulmonary fibrosis, examines the predictors of survival in this cohort of patients, and explores the impact of palliative care on survival. <b>Design:</b> Charts were reviewed retrospectively and analyzed. The primary outcome was survival during a 4-year follow-up period. Two multivariable models were created to examine the impact of therapeutic strategies including palliative intervention on survival. <b>Results:</b> 298 patients with idiopathic pulmonary fibrosis were enrolled from 3 interstitial lung disease clinics with different palliative care models in Edmonton, Canada; Bristol, UK; and Kingston, Canada. 200 (67%) patients received palliative care and 119 (40%) died during follow up. Primary palliative care models (Edmonton and Bristol) delivered palliative care to 96% and 100% respectively compared 21% in the referral model (Queens). Palliative care [adjusted hazard ratio (aHR) .28 (.12-.65)] along with the use of antifibrotics [aHR .56 (.37-.84)], and body mass index >30 [aHR .47 (.37-.85)] reduced the risk of death in our idiopathic pulmonary fibrosis cohort. Opioid use was associated with worse survival [aHR 2.11 (1.30-23.43)]. <b>Conclusions:</b> Both palliative care and antifibrotic use were associated with survival benefit in this cohort of patients with idiopathic pulmonary fibrosis after adjusting for covariates. The benefit was seen despite differences in disease severity and different palliative care delivery models.</p>","PeriodicalId":50810,"journal":{"name":"American Journal of Hospice & Palliative Medicine","volume":" ","pages":"610-618"},"PeriodicalIF":1.4000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11032628/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Impact of Integrated Palliative Care on Survival in Idiopathic Pulmonary Fibrosis: A Retrospective Multicenter Comparison.\",\"authors\":\"Jenny Lu-Song, Jeffrey A Bakal, Sarah Younus, Onofre Moran-Mendoza, Ingrid Harle, Michelle Morales, Naomi Rippon, Shaney L Barratt, Huzaifa Adamali, Meena Kalluri\",\"doi\":\"10.1177/10499091231194722\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Early and integrated palliative care is recommended for patients with idiopathic pulmonary fibrosis. Unfortunately, palliative care delivery remains poor due to various barriers in practice. This study describes various palliative care delivery models in a real-world cohort of patients with idiopathic pulmonary fibrosis, examines the predictors of survival in this cohort of patients, and explores the impact of palliative care on survival. <b>Design:</b> Charts were reviewed retrospectively and analyzed. The primary outcome was survival during a 4-year follow-up period. Two multivariable models were created to examine the impact of therapeutic strategies including palliative intervention on survival. <b>Results:</b> 298 patients with idiopathic pulmonary fibrosis were enrolled from 3 interstitial lung disease clinics with different palliative care models in Edmonton, Canada; Bristol, UK; and Kingston, Canada. 200 (67%) patients received palliative care and 119 (40%) died during follow up. Primary palliative care models (Edmonton and Bristol) delivered palliative care to 96% and 100% respectively compared 21% in the referral model (Queens). Palliative care [adjusted hazard ratio (aHR) .28 (.12-.65)] along with the use of antifibrotics [aHR .56 (.37-.84)], and body mass index >30 [aHR .47 (.37-.85)] reduced the risk of death in our idiopathic pulmonary fibrosis cohort. Opioid use was associated with worse survival [aHR 2.11 (1.30-23.43)]. <b>Conclusions:</b> Both palliative care and antifibrotic use were associated with survival benefit in this cohort of patients with idiopathic pulmonary fibrosis after adjusting for covariates. The benefit was seen despite differences in disease severity and different palliative care delivery models.</p>\",\"PeriodicalId\":50810,\"journal\":{\"name\":\"American Journal of Hospice & Palliative Medicine\",\"volume\":\" \",\"pages\":\"610-618\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11032628/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Hospice & Palliative Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/10499091231194722\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/8/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hospice & Palliative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/10499091231194722","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/8 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
The Impact of Integrated Palliative Care on Survival in Idiopathic Pulmonary Fibrosis: A Retrospective Multicenter Comparison.
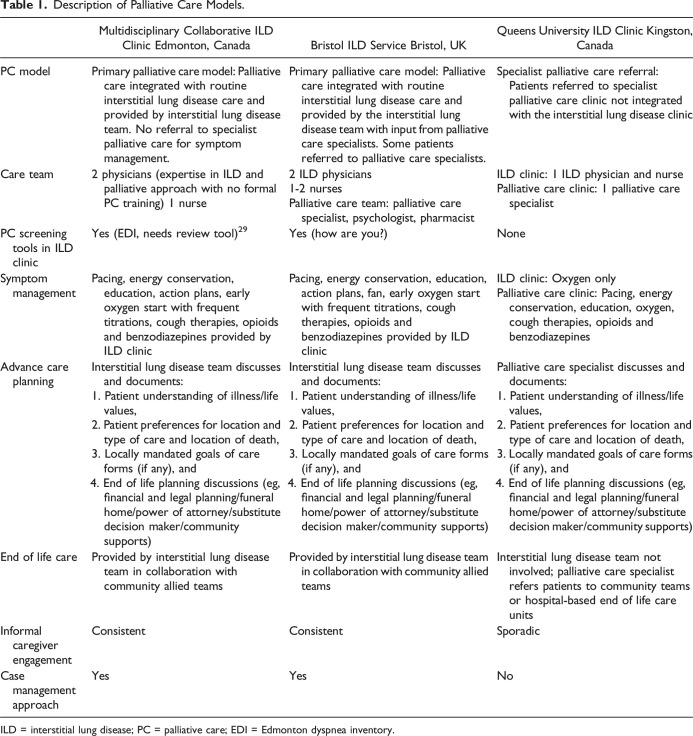
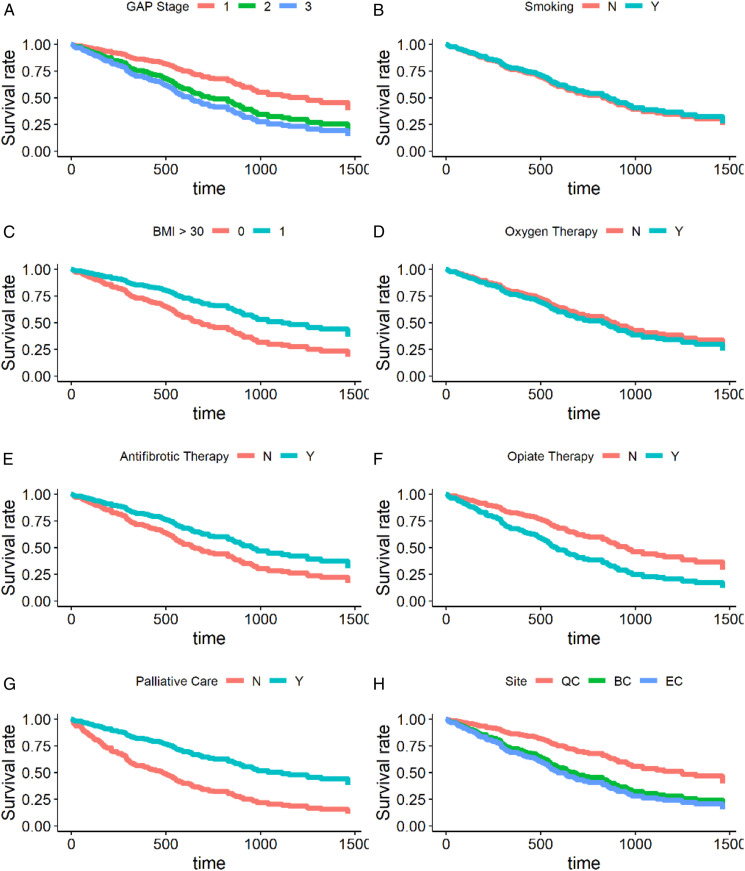
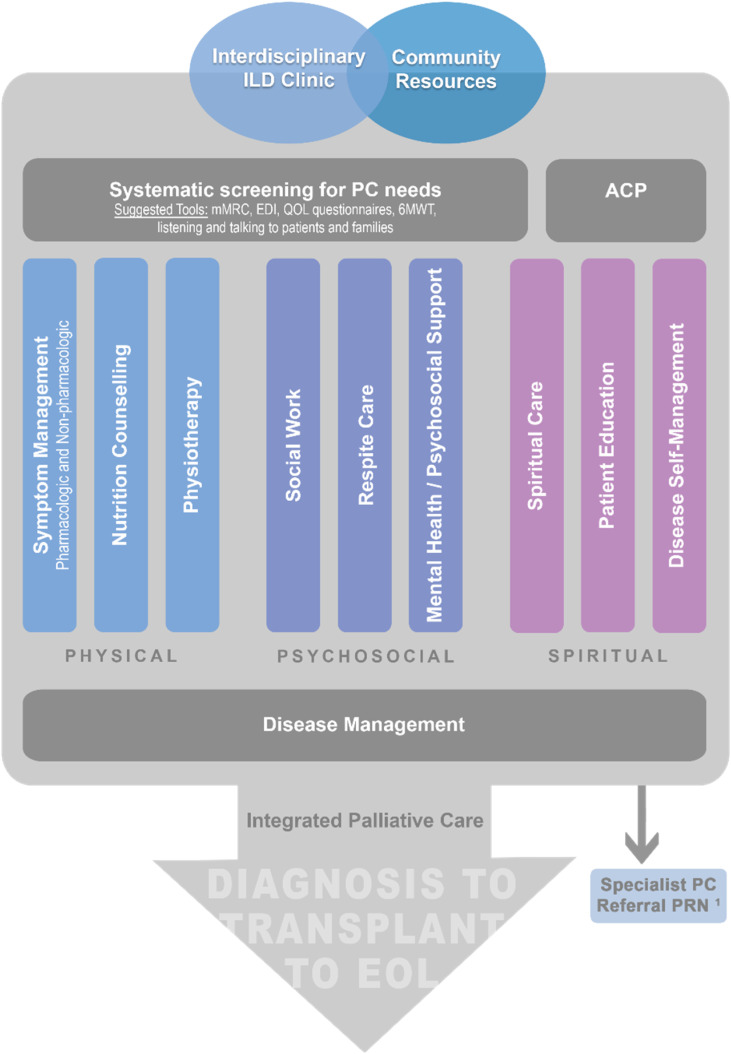
Background: Early and integrated palliative care is recommended for patients with idiopathic pulmonary fibrosis. Unfortunately, palliative care delivery remains poor due to various barriers in practice. This study describes various palliative care delivery models in a real-world cohort of patients with idiopathic pulmonary fibrosis, examines the predictors of survival in this cohort of patients, and explores the impact of palliative care on survival. Design: Charts were reviewed retrospectively and analyzed. The primary outcome was survival during a 4-year follow-up period. Two multivariable models were created to examine the impact of therapeutic strategies including palliative intervention on survival. Results: 298 patients with idiopathic pulmonary fibrosis were enrolled from 3 interstitial lung disease clinics with different palliative care models in Edmonton, Canada; Bristol, UK; and Kingston, Canada. 200 (67%) patients received palliative care and 119 (40%) died during follow up. Primary palliative care models (Edmonton and Bristol) delivered palliative care to 96% and 100% respectively compared 21% in the referral model (Queens). Palliative care [adjusted hazard ratio (aHR) .28 (.12-.65)] along with the use of antifibrotics [aHR .56 (.37-.84)], and body mass index >30 [aHR .47 (.37-.85)] reduced the risk of death in our idiopathic pulmonary fibrosis cohort. Opioid use was associated with worse survival [aHR 2.11 (1.30-23.43)]. Conclusions: Both palliative care and antifibrotic use were associated with survival benefit in this cohort of patients with idiopathic pulmonary fibrosis after adjusting for covariates. The benefit was seen despite differences in disease severity and different palliative care delivery models.
期刊介绍:
American Journal of Hospice & Palliative Medicine (AJHPM) is a peer-reviewed journal, published eight times a year. In 30 years of publication, AJHPM has highlighted the interdisciplinary team approach to hospice and palliative medicine as related to the care of the patient and family. This journal is a member of the Committee on Publication Ethics (COPE).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


