Yukiharu Sugimura, Moritz Benjamin Immohr, Arash Mehdiani, Udo Boeken, Hug Aubin, Artur Lichtenberg, Payam Akhyari
{"title":"Impella 支持对心肌梗死术后心源性休克患者临床疗效的影响。","authors":"Yukiharu Sugimura, Moritz Benjamin Immohr, Arash Mehdiani, Udo Boeken, Hug Aubin, Artur Lichtenberg, Payam Akhyari","doi":"10.5761/atcs.oa.23-00076","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to elucidate the strategy of an effective Impella support for better clinical outcomes in patients with a postcardiotomy cardiogenic shock (PCCS).</p><p><strong>Methods: </strong>This single-center retrospective observational study enrolled 31 patients with PCCS undergoing an elective open-heart surgery followed by Impella support between November 2018 and February 2022 for further analysis.</p><p><strong>Results: </strong>The preoperative Euroscore II and left ventricular (LV) ejection fraction were 9.1 ± 10.4 and 35.7% ± 12.6%, respectively. The in-hospital mortality rate was 51.6% (n = 16). In survivors (n = 15), the mean Impella support time was 6.9 ± 3.5 days. Patients were discharged on the postoperative day 24.9 ± 16.4. Regarding LV remodeling, LV end-diastolic diameter was significantly decreased after Impella support (59.2 ± 6.0 mm vs. 54.4 ± 4.7 mm, p = 0.01, preoperative vs. postoperative). In-hospital mortality rates were comparable with small (CP, n = 6) or large (5.0, n = 25) Impella systems (33.3% [n = 2] vs. 56.0% [n = 14], p = 0.39). However, a lower in-hospital mortality rate was observed in the group with early initiation (i.e., intraoperative) of Impella support (n = 14) than that with delayed Impella initiation (i.e., in the postoperative course) (n = 11) (28.6% [n = 4] vs. 90.9% [n = 10], p = 0.004).</p><p><strong>Conclusions: </strong>Impella support contributes to LV remodeling in PCCS patients. In-hospital mortality was comparable in different Impella sizes and lower in early Impella initiation.</p>","PeriodicalId":8037,"journal":{"name":"Annals of Thoracic and Cardiovascular Surgery","volume":" ","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2024-01-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10902663/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of Impella Support on Clinical Outcomes in Patients with Postcardiotomy Cardiogenic Shock.\",\"authors\":\"Yukiharu Sugimura, Moritz Benjamin Immohr, Arash Mehdiani, Udo Boeken, Hug Aubin, Artur Lichtenberg, Payam Akhyari\",\"doi\":\"10.5761/atcs.oa.23-00076\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>This study aimed to elucidate the strategy of an effective Impella support for better clinical outcomes in patients with a postcardiotomy cardiogenic shock (PCCS).</p><p><strong>Methods: </strong>This single-center retrospective observational study enrolled 31 patients with PCCS undergoing an elective open-heart surgery followed by Impella support between November 2018 and February 2022 for further analysis.</p><p><strong>Results: </strong>The preoperative Euroscore II and left ventricular (LV) ejection fraction were 9.1 ± 10.4 and 35.7% ± 12.6%, respectively. The in-hospital mortality rate was 51.6% (n = 16). In survivors (n = 15), the mean Impella support time was 6.9 ± 3.5 days. Patients were discharged on the postoperative day 24.9 ± 16.4. Regarding LV remodeling, LV end-diastolic diameter was significantly decreased after Impella support (59.2 ± 6.0 mm vs. 54.4 ± 4.7 mm, p = 0.01, preoperative vs. postoperative). In-hospital mortality rates were comparable with small (CP, n = 6) or large (5.0, n = 25) Impella systems (33.3% [n = 2] vs. 56.0% [n = 14], p = 0.39). However, a lower in-hospital mortality rate was observed in the group with early initiation (i.e., intraoperative) of Impella support (n = 14) than that with delayed Impella initiation (i.e., in the postoperative course) (n = 11) (28.6% [n = 4] vs. 90.9% [n = 10], p = 0.004).</p><p><strong>Conclusions: </strong>Impella support contributes to LV remodeling in PCCS patients. In-hospital mortality was comparable in different Impella sizes and lower in early Impella initiation.</p>\",\"PeriodicalId\":8037,\"journal\":{\"name\":\"Annals of Thoracic and Cardiovascular Surgery\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-01-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10902663/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5761/atcs.oa.23-00076\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/8/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.oa.23-00076","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/3 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Impact of Impella Support on Clinical Outcomes in Patients with Postcardiotomy Cardiogenic Shock.
Purpose: This study aimed to elucidate the strategy of an effective Impella support for better clinical outcomes in patients with a postcardiotomy cardiogenic shock (PCCS).
Methods: This single-center retrospective observational study enrolled 31 patients with PCCS undergoing an elective open-heart surgery followed by Impella support between November 2018 and February 2022 for further analysis.
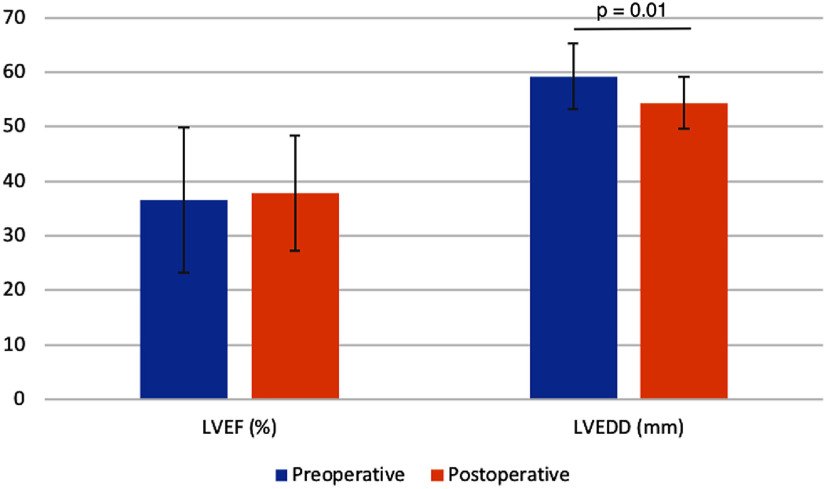
Results: The preoperative Euroscore II and left ventricular (LV) ejection fraction were 9.1 ± 10.4 and 35.7% ± 12.6%, respectively. The in-hospital mortality rate was 51.6% (n = 16). In survivors (n = 15), the mean Impella support time was 6.9 ± 3.5 days. Patients were discharged on the postoperative day 24.9 ± 16.4. Regarding LV remodeling, LV end-diastolic diameter was significantly decreased after Impella support (59.2 ± 6.0 mm vs. 54.4 ± 4.7 mm, p = 0.01, preoperative vs. postoperative). In-hospital mortality rates were comparable with small (CP, n = 6) or large (5.0, n = 25) Impella systems (33.3% [n = 2] vs. 56.0% [n = 14], p = 0.39). However, a lower in-hospital mortality rate was observed in the group with early initiation (i.e., intraoperative) of Impella support (n = 14) than that with delayed Impella initiation (i.e., in the postoperative course) (n = 11) (28.6% [n = 4] vs. 90.9% [n = 10], p = 0.004).
Conclusions: Impella support contributes to LV remodeling in PCCS patients. In-hospital mortality was comparable in different Impella sizes and lower in early Impella initiation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


