Chiara Alfia Ferrara, Gaetano La Rocca, Giuseppe Ielo, Alessandro Libra, Gianluca Sambataro
{"title":"混合性结缔组织病的早期诊断:最新观点。","authors":"Chiara Alfia Ferrara, Gaetano La Rocca, Giuseppe Ielo, Alessandro Libra, Gianluca Sambataro","doi":"10.2147/ITT.S390023","DOIUrl":null,"url":null,"abstract":"<p><p>Mixed Connective Tissue Disease (MCTD) is an autoimmune disease first described by Sharp et al in 1972, characterized by the presence of anti-Ribonucleoprotein antibodies directed against the U1 complex (anti-U1RNP). The condition shares clinical characteristics with Systemic Lupus Erythematosus, Rheumatoid Arthritis, and Systemic Sclerosis. Diagnosis is quite difficult due to its rarity, the lack of validated classification criteria, and its heterogeneous clinical presentation. While in the early stages its nuanced clinical features might lead to it being incorrectly classified as other Connective Tissue Diseases (CTDs) or even not recognized, in cases of longstanding disease its classification as a CTD is clear but challenging to discriminate from overlap syndromes. MCTD should be considered a distinct entity due to the presence of a specific genetic substrate and the presence of the high titer of a specific autoantibody, anti-U1RNP, present in all the commercial kits for Extractable Nuclear Antigens, and almost always associated with Antinuclear Antibody positivity with a coarse speckled pattern. Except for anti-U1RNP, no specific biomarkers are available to guide clinicians to a correct classification of MCTD, which is arrived at by the association of clinical, serological and instrumental evaluation. In the first stages, the disease is mainly characterized by Raynaud's phenomenon, inflammatory arthritis, puffy fingers, myalgia and/or myositis, and rarely, trigeminal neuropathy. Longstanding disease is generally associated with the development of Pulmonary Hypertension and Interstitial Lung Disease, which are the two main causes of mortality in MCTD. The aim of this review is to summarize current knowledge on the early recognition of MCTD.</p>","PeriodicalId":30986,"journal":{"name":"ImmunoTargets and Therapy","volume":"12 ","pages":"79-89"},"PeriodicalIF":6.2000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/04/39/itt-12-79.PMC10387239.pdf","citationCount":"0","resultStr":"{\"title\":\"Towards Early Diagnosis of Mixed Connective Tissue Disease: Updated Perspectives.\",\"authors\":\"Chiara Alfia Ferrara, Gaetano La Rocca, Giuseppe Ielo, Alessandro Libra, Gianluca Sambataro\",\"doi\":\"10.2147/ITT.S390023\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Mixed Connective Tissue Disease (MCTD) is an autoimmune disease first described by Sharp et al in 1972, characterized by the presence of anti-Ribonucleoprotein antibodies directed against the U1 complex (anti-U1RNP). The condition shares clinical characteristics with Systemic Lupus Erythematosus, Rheumatoid Arthritis, and Systemic Sclerosis. Diagnosis is quite difficult due to its rarity, the lack of validated classification criteria, and its heterogeneous clinical presentation. While in the early stages its nuanced clinical features might lead to it being incorrectly classified as other Connective Tissue Diseases (CTDs) or even not recognized, in cases of longstanding disease its classification as a CTD is clear but challenging to discriminate from overlap syndromes. MCTD should be considered a distinct entity due to the presence of a specific genetic substrate and the presence of the high titer of a specific autoantibody, anti-U1RNP, present in all the commercial kits for Extractable Nuclear Antigens, and almost always associated with Antinuclear Antibody positivity with a coarse speckled pattern. Except for anti-U1RNP, no specific biomarkers are available to guide clinicians to a correct classification of MCTD, which is arrived at by the association of clinical, serological and instrumental evaluation. In the first stages, the disease is mainly characterized by Raynaud's phenomenon, inflammatory arthritis, puffy fingers, myalgia and/or myositis, and rarely, trigeminal neuropathy. Longstanding disease is generally associated with the development of Pulmonary Hypertension and Interstitial Lung Disease, which are the two main causes of mortality in MCTD. The aim of this review is to summarize current knowledge on the early recognition of MCTD.</p>\",\"PeriodicalId\":30986,\"journal\":{\"name\":\"ImmunoTargets and Therapy\",\"volume\":\"12 \",\"pages\":\"79-89\"},\"PeriodicalIF\":6.2000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/04/39/itt-12-79.PMC10387239.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ImmunoTargets and Therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/ITT.S390023\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ImmunoTargets and Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/ITT.S390023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Towards Early Diagnosis of Mixed Connective Tissue Disease: Updated Perspectives.
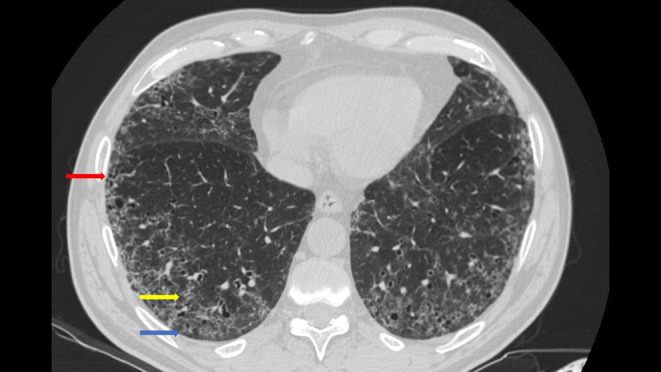
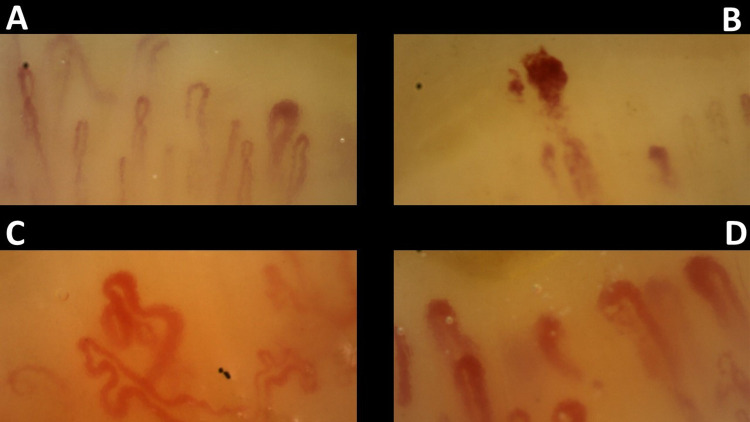
Mixed Connective Tissue Disease (MCTD) is an autoimmune disease first described by Sharp et al in 1972, characterized by the presence of anti-Ribonucleoprotein antibodies directed against the U1 complex (anti-U1RNP). The condition shares clinical characteristics with Systemic Lupus Erythematosus, Rheumatoid Arthritis, and Systemic Sclerosis. Diagnosis is quite difficult due to its rarity, the lack of validated classification criteria, and its heterogeneous clinical presentation. While in the early stages its nuanced clinical features might lead to it being incorrectly classified as other Connective Tissue Diseases (CTDs) or even not recognized, in cases of longstanding disease its classification as a CTD is clear but challenging to discriminate from overlap syndromes. MCTD should be considered a distinct entity due to the presence of a specific genetic substrate and the presence of the high titer of a specific autoantibody, anti-U1RNP, present in all the commercial kits for Extractable Nuclear Antigens, and almost always associated with Antinuclear Antibody positivity with a coarse speckled pattern. Except for anti-U1RNP, no specific biomarkers are available to guide clinicians to a correct classification of MCTD, which is arrived at by the association of clinical, serological and instrumental evaluation. In the first stages, the disease is mainly characterized by Raynaud's phenomenon, inflammatory arthritis, puffy fingers, myalgia and/or myositis, and rarely, trigeminal neuropathy. Longstanding disease is generally associated with the development of Pulmonary Hypertension and Interstitial Lung Disease, which are the two main causes of mortality in MCTD. The aim of this review is to summarize current knowledge on the early recognition of MCTD.
期刊介绍:
Immuno Targets and Therapy is an international, peer-reviewed open access journal focusing on the immunological basis of diseases, potential targets for immune based therapy and treatment protocols employed to improve patient management. Basic immunology and physiology of the immune system in health, and disease will be also covered.In addition, the journal will focus on the impact of management programs and new therapeutic agents and protocols on patient perspectives such as quality of life, adherence and satisfaction.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


