Prina Donga, Bruno Emond, Carmine Rossi, Brahim K Bookhart, Johnnie Lee, Gabrielle Caron-Lapointe, Fangzhou Wei, Marie-Hélène Lafeuille
{"title":"超重或肥胖(ART-Naïve) HIV-1感染者开始使用恩曲他滨/替诺福韦阿拉胺与达鲁那韦合用或与多替格拉韦合用后体重和BMI的变化","authors":"Prina Donga, Bruno Emond, Carmine Rossi, Brahim K Bookhart, Johnnie Lee, Gabrielle Caron-Lapointe, Fangzhou Wei, Marie-Hélène Lafeuille","doi":"10.2147/CEOR.S413800","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Integrase strand transfer inhibitor-based regimens (eg, containing dolutegravir [DTG]) are associated with weight/body mass index (BMI) increases among people living with HIV-1 (PLWH). Assessing antiretroviral therapy (ART)-related weight/BMI changes is challenging, as PLWH may experience return-to-health weight gain as a result of viral suppression. This retrospective, longitudinal real-world study compared weight/BMI outcomes among overweight/obese (BMI ≥25 kg/m<sup>2</sup>; thus excluding return-to-health weight/BMI changes), treatment-naïve PLWH who initiated darunavir (DRV)/cobicistat (c)/emtricitabine (FTC)/tenofovir alafenamide (TAF) or DTG + FTC/TAF.</p><p><strong>Methods: </strong>Treatment-naïve PLWH with BMI ≥25 kg/m<sup>2</sup> who initiated DRV/c/FTC/TAF or DTG + FTC/TAF (index date) had ≥12 months of baseline observation and ≥1 weight/BMI measurement in baseline and post-index periods in the Symphony Health IDV<sup>®</sup> database (07/17/2017-12/31/2021) were included. Inverse probability of treatment weighting (IPTW) was used to balance differences in baseline characteristics between cohorts. On-treatment time-to-weight/BMI increases ≥5% were compared between cohorts using weighted adjusted Cox models.</p><p><strong>Results: </strong>Post-IPTW, 76 overweight/obese DRV/c/FTC/TAF-treated (mean age = 51.2 years, 30.7% female, 35.6% Black, mean baseline BMI = 33.2 kg/m<sup>2</sup>) and 88 overweight/obese DTG + FTC/TAF-treated PLWH (mean age = 51.5 years, 31.4% female, 31.4% Black, mean baseline BMI = 32.7 kg/m<sup>2</sup>) were included. The median [interquartile range] time from ART initiation to weight/BMI increase ≥5% was shorter for the DTG + FTC/TAF cohort (21.8 [9.9, 32.3] months) than the DRV/c/FTC/TAF cohort (median and interquartile times not reached; Kaplan-Meier rate at 21.8 months = 20.8%). Over the entire follow-up, overweight/obese PLWH initiating DTG + FTC/TAF had a more than twofold greater risk of experiencing weight/BMI increase ≥5% compared to those initiating DRV/c/FTC/TAF (hazard ratio [95% confidence interval]=2.43 [1.02; 7.04]; p = 0.036).</p><p><strong>Conclusion: </strong>Overweight/obese PLWH who initiated DTG + FTC/TAF had significantly greater risk of weight/BMI increase ≥5% compared to similar PLWH who initiated DRV/c/FTC/TAF and had shorter time-to-weight/BMI increase ≥5%, suggesting a need for additional monitoring to assess the risk of weight gain-related cardiometabolic disease.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"15 ","pages":"579-591"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dd/80/ceor-15-579.PMC10377594.pdf","citationCount":"1","resultStr":"{\"title\":\"Weight and BMI Changes Following Initiation of Emtricitabine/Tenofovir Alafenamide Co-Formulated with Darunavir or Co-Administered with Dolutegravir in Overweight or Obese, ART-Naïve People Living with HIV-1.\",\"authors\":\"Prina Donga, Bruno Emond, Carmine Rossi, Brahim K Bookhart, Johnnie Lee, Gabrielle Caron-Lapointe, Fangzhou Wei, Marie-Hélène Lafeuille\",\"doi\":\"10.2147/CEOR.S413800\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Integrase strand transfer inhibitor-based regimens (eg, containing dolutegravir [DTG]) are associated with weight/body mass index (BMI) increases among people living with HIV-1 (PLWH). Assessing antiretroviral therapy (ART)-related weight/BMI changes is challenging, as PLWH may experience return-to-health weight gain as a result of viral suppression. This retrospective, longitudinal real-world study compared weight/BMI outcomes among overweight/obese (BMI ≥25 kg/m<sup>2</sup>; thus excluding return-to-health weight/BMI changes), treatment-naïve PLWH who initiated darunavir (DRV)/cobicistat (c)/emtricitabine (FTC)/tenofovir alafenamide (TAF) or DTG + FTC/TAF.</p><p><strong>Methods: </strong>Treatment-naïve PLWH with BMI ≥25 kg/m<sup>2</sup> who initiated DRV/c/FTC/TAF or DTG + FTC/TAF (index date) had ≥12 months of baseline observation and ≥1 weight/BMI measurement in baseline and post-index periods in the Symphony Health IDV<sup>®</sup> database (07/17/2017-12/31/2021) were included. Inverse probability of treatment weighting (IPTW) was used to balance differences in baseline characteristics between cohorts. On-treatment time-to-weight/BMI increases ≥5% were compared between cohorts using weighted adjusted Cox models.</p><p><strong>Results: </strong>Post-IPTW, 76 overweight/obese DRV/c/FTC/TAF-treated (mean age = 51.2 years, 30.7% female, 35.6% Black, mean baseline BMI = 33.2 kg/m<sup>2</sup>) and 88 overweight/obese DTG + FTC/TAF-treated PLWH (mean age = 51.5 years, 31.4% female, 31.4% Black, mean baseline BMI = 32.7 kg/m<sup>2</sup>) were included. The median [interquartile range] time from ART initiation to weight/BMI increase ≥5% was shorter for the DTG + FTC/TAF cohort (21.8 [9.9, 32.3] months) than the DRV/c/FTC/TAF cohort (median and interquartile times not reached; Kaplan-Meier rate at 21.8 months = 20.8%). Over the entire follow-up, overweight/obese PLWH initiating DTG + FTC/TAF had a more than twofold greater risk of experiencing weight/BMI increase ≥5% compared to those initiating DRV/c/FTC/TAF (hazard ratio [95% confidence interval]=2.43 [1.02; 7.04]; p = 0.036).</p><p><strong>Conclusion: </strong>Overweight/obese PLWH who initiated DTG + FTC/TAF had significantly greater risk of weight/BMI increase ≥5% compared to similar PLWH who initiated DRV/c/FTC/TAF and had shorter time-to-weight/BMI increase ≥5%, suggesting a need for additional monitoring to assess the risk of weight gain-related cardiometabolic disease.</p>\",\"PeriodicalId\":47313,\"journal\":{\"name\":\"ClinicoEconomics and Outcomes Research\",\"volume\":\"15 \",\"pages\":\"579-591\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dd/80/ceor-15-579.PMC10377594.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ClinicoEconomics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEOR.S413800\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S413800","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Weight and BMI Changes Following Initiation of Emtricitabine/Tenofovir Alafenamide Co-Formulated with Darunavir or Co-Administered with Dolutegravir in Overweight or Obese, ART-Naïve People Living with HIV-1.
Introduction: Integrase strand transfer inhibitor-based regimens (eg, containing dolutegravir [DTG]) are associated with weight/body mass index (BMI) increases among people living with HIV-1 (PLWH). Assessing antiretroviral therapy (ART)-related weight/BMI changes is challenging, as PLWH may experience return-to-health weight gain as a result of viral suppression. This retrospective, longitudinal real-world study compared weight/BMI outcomes among overweight/obese (BMI ≥25 kg/m2; thus excluding return-to-health weight/BMI changes), treatment-naïve PLWH who initiated darunavir (DRV)/cobicistat (c)/emtricitabine (FTC)/tenofovir alafenamide (TAF) or DTG + FTC/TAF.
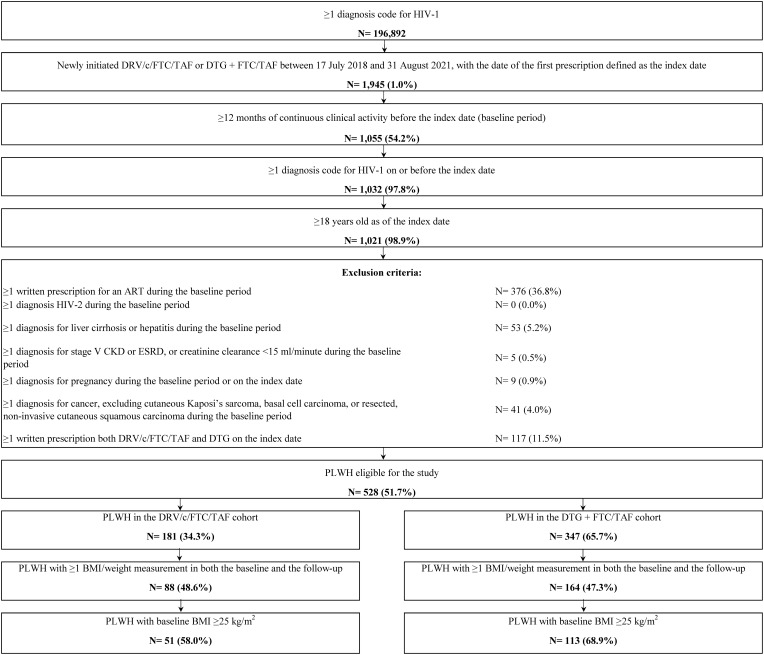
Methods: Treatment-naïve PLWH with BMI ≥25 kg/m2 who initiated DRV/c/FTC/TAF or DTG + FTC/TAF (index date) had ≥12 months of baseline observation and ≥1 weight/BMI measurement in baseline and post-index periods in the Symphony Health IDV® database (07/17/2017-12/31/2021) were included. Inverse probability of treatment weighting (IPTW) was used to balance differences in baseline characteristics between cohorts. On-treatment time-to-weight/BMI increases ≥5% were compared between cohorts using weighted adjusted Cox models.
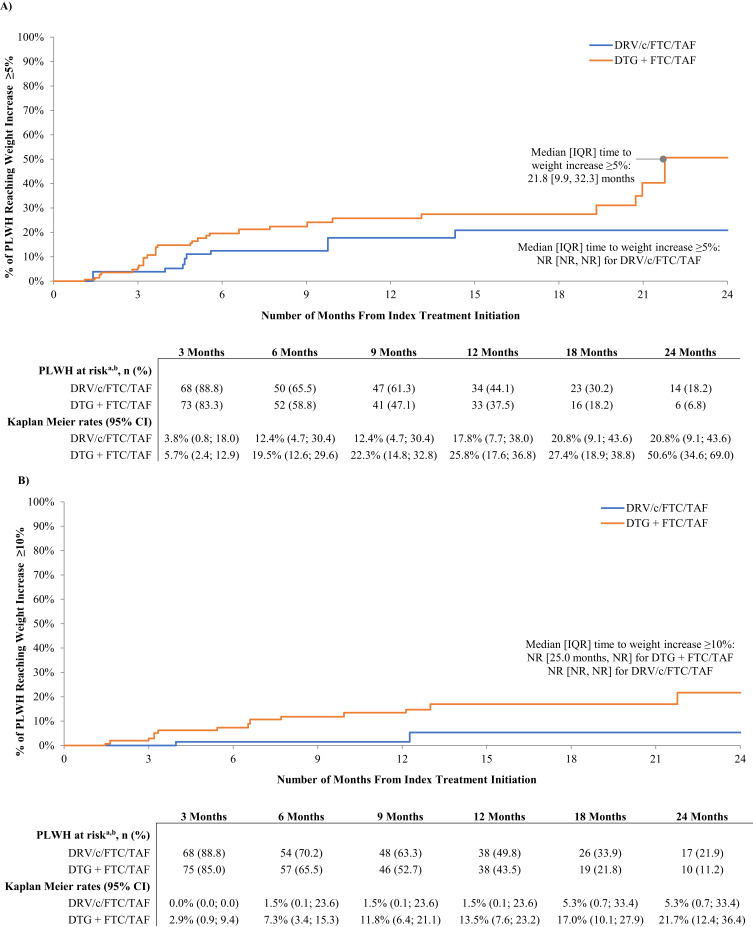
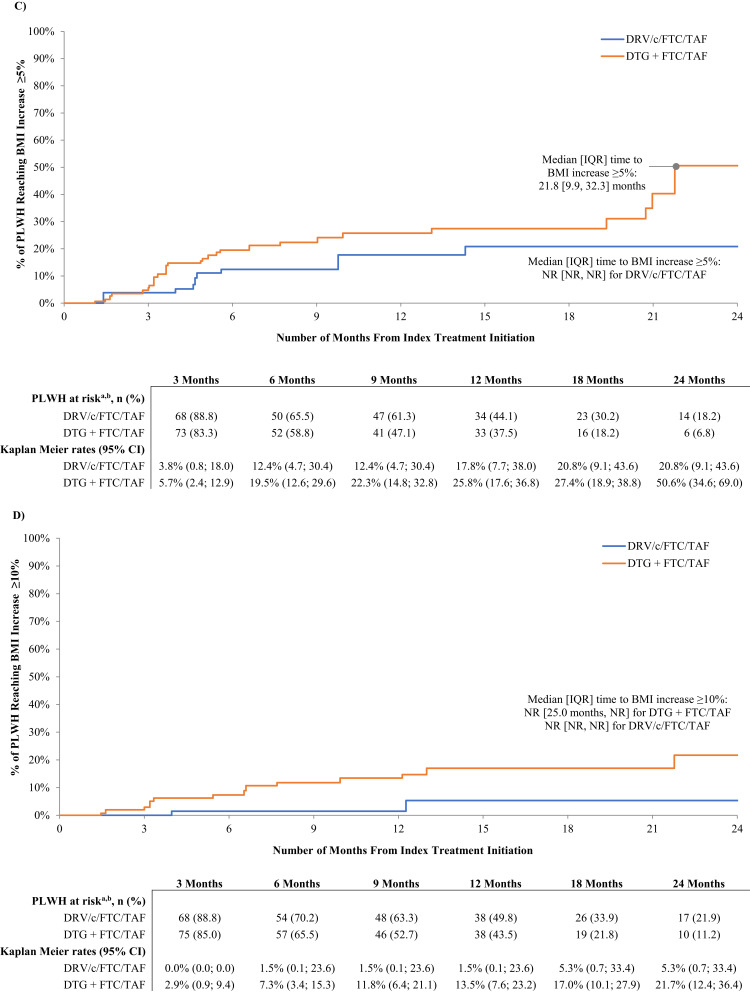
Results: Post-IPTW, 76 overweight/obese DRV/c/FTC/TAF-treated (mean age = 51.2 years, 30.7% female, 35.6% Black, mean baseline BMI = 33.2 kg/m2) and 88 overweight/obese DTG + FTC/TAF-treated PLWH (mean age = 51.5 years, 31.4% female, 31.4% Black, mean baseline BMI = 32.7 kg/m2) were included. The median [interquartile range] time from ART initiation to weight/BMI increase ≥5% was shorter for the DTG + FTC/TAF cohort (21.8 [9.9, 32.3] months) than the DRV/c/FTC/TAF cohort (median and interquartile times not reached; Kaplan-Meier rate at 21.8 months = 20.8%). Over the entire follow-up, overweight/obese PLWH initiating DTG + FTC/TAF had a more than twofold greater risk of experiencing weight/BMI increase ≥5% compared to those initiating DRV/c/FTC/TAF (hazard ratio [95% confidence interval]=2.43 [1.02; 7.04]; p = 0.036).
Conclusion: Overweight/obese PLWH who initiated DTG + FTC/TAF had significantly greater risk of weight/BMI increase ≥5% compared to similar PLWH who initiated DRV/c/FTC/TAF and had shorter time-to-weight/BMI increase ≥5%, suggesting a need for additional monitoring to assess the risk of weight gain-related cardiometabolic disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


