Maulik K Lathiya, Praveen Errabelli, Salvatore Mignano, Susan M Cullinan
{"title":"无形体病继发于感染相关膜增生性肾小球肾炎1例。","authors":"Maulik K Lathiya, Praveen Errabelli, Salvatore Mignano, Susan M Cullinan","doi":"10.5527/wjn.v12.i3.66","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anaplasmosis is a tick-borne disease with a range of clinical manifestations, from a flu-like illness with fever and myalgias to a severe systemic disease with multisystem organ failure. Although renal involvement is not a common presentation, there have been few cases reporting acute kidney injury from Anaplasmosis.</p><p><strong>Case summary: </strong>We present a 55-year-old female with anaplasmosis who developed acute kidney injury due to membranoproliferative glomerulonephritis (MPGN). The patient originally presented with cough and shortness of breath. She was admitted to the hospital with a diagnosis of community acquired pneumonia and received antibiotics. During the hospital course she developed severe acute renal failure. Initial serological work up didn't provide any conclusive diagnosis. Hence, she underwent kidney biopsy which showed MPGN pattern suggesting autoimmune, multiple myeloma or infectious etiology. Extensive work up was undertaken which was negative for autoimmune diseases, vasculitis panel, paraproteinemias but tested positive for IgG anaplasma with high titers indicating Anaplasmosis.</p><p><strong>Conclusion: </strong>Our case shows a unique presentation of severe acute renal failure from MPGN from tick borne illness. MPGN is usually seen with autoimmune diseases, hepatitis C virus infections, paraproteinemias. Hence, we suggest that tick borne illness should also be considered when evaluating acute renal failure cases in tick borne prevalent regions.</p>","PeriodicalId":23745,"journal":{"name":"World Journal of Nephrology","volume":"12 3","pages":"66-72"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c5/fb/WJN-12-66.PMC10354567.pdf","citationCount":"0","resultStr":"{\"title\":\"Infection related membranoproliferative glomerulonephritis secondary to anaplasmosis: A case report.\",\"authors\":\"Maulik K Lathiya, Praveen Errabelli, Salvatore Mignano, Susan M Cullinan\",\"doi\":\"10.5527/wjn.v12.i3.66\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Anaplasmosis is a tick-borne disease with a range of clinical manifestations, from a flu-like illness with fever and myalgias to a severe systemic disease with multisystem organ failure. Although renal involvement is not a common presentation, there have been few cases reporting acute kidney injury from Anaplasmosis.</p><p><strong>Case summary: </strong>We present a 55-year-old female with anaplasmosis who developed acute kidney injury due to membranoproliferative glomerulonephritis (MPGN). The patient originally presented with cough and shortness of breath. She was admitted to the hospital with a diagnosis of community acquired pneumonia and received antibiotics. During the hospital course she developed severe acute renal failure. Initial serological work up didn't provide any conclusive diagnosis. Hence, she underwent kidney biopsy which showed MPGN pattern suggesting autoimmune, multiple myeloma or infectious etiology. Extensive work up was undertaken which was negative for autoimmune diseases, vasculitis panel, paraproteinemias but tested positive for IgG anaplasma with high titers indicating Anaplasmosis.</p><p><strong>Conclusion: </strong>Our case shows a unique presentation of severe acute renal failure from MPGN from tick borne illness. MPGN is usually seen with autoimmune diseases, hepatitis C virus infections, paraproteinemias. Hence, we suggest that tick borne illness should also be considered when evaluating acute renal failure cases in tick borne prevalent regions.</p>\",\"PeriodicalId\":23745,\"journal\":{\"name\":\"World Journal of Nephrology\",\"volume\":\"12 3\",\"pages\":\"66-72\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-05-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c5/fb/WJN-12-66.PMC10354567.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Nephrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5527/wjn.v12.i3.66\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5527/wjn.v12.i3.66","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Infection related membranoproliferative glomerulonephritis secondary to anaplasmosis: A case report.
Background: Anaplasmosis is a tick-borne disease with a range of clinical manifestations, from a flu-like illness with fever and myalgias to a severe systemic disease with multisystem organ failure. Although renal involvement is not a common presentation, there have been few cases reporting acute kidney injury from Anaplasmosis.
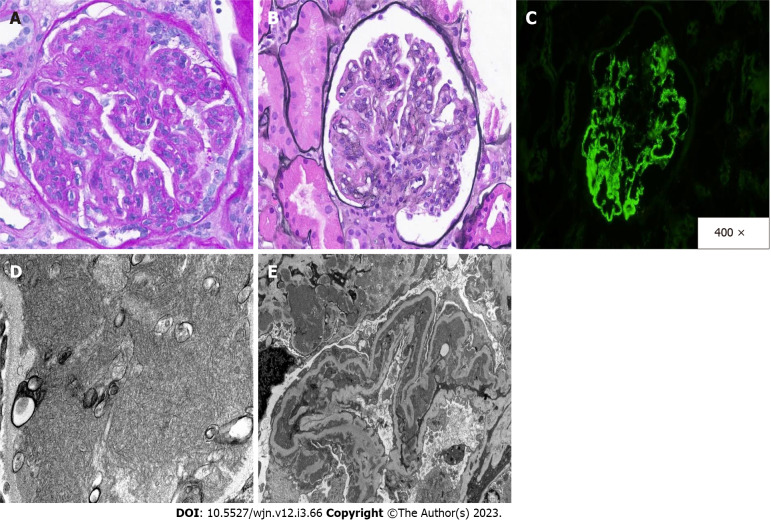
Case summary: We present a 55-year-old female with anaplasmosis who developed acute kidney injury due to membranoproliferative glomerulonephritis (MPGN). The patient originally presented with cough and shortness of breath. She was admitted to the hospital with a diagnosis of community acquired pneumonia and received antibiotics. During the hospital course she developed severe acute renal failure. Initial serological work up didn't provide any conclusive diagnosis. Hence, she underwent kidney biopsy which showed MPGN pattern suggesting autoimmune, multiple myeloma or infectious etiology. Extensive work up was undertaken which was negative for autoimmune diseases, vasculitis panel, paraproteinemias but tested positive for IgG anaplasma with high titers indicating Anaplasmosis.
Conclusion: Our case shows a unique presentation of severe acute renal failure from MPGN from tick borne illness. MPGN is usually seen with autoimmune diseases, hepatitis C virus infections, paraproteinemias. Hence, we suggest that tick borne illness should also be considered when evaluating acute renal failure cases in tick borne prevalent regions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


