Jordan Willis, Stephanie Jarvis, Gina M Berg, Chad Corrigan, Robert Madayag, Cassandra Reynolds, Allen Tanner, Gary Marshall, Carlos Palacio Lascano, David Bar-Or
{"title":"限制性液体治疗对老年髋部骨折预后的影响:一项来自5个一级创伤中心的回顾性队列研究","authors":"Jordan Willis, Stephanie Jarvis, Gina M Berg, Chad Corrigan, Robert Madayag, Cassandra Reynolds, Allen Tanner, Gary Marshall, Carlos Palacio Lascano, David Bar-Or","doi":"10.1097/OI9.0000000000000279","DOIUrl":null,"url":null,"abstract":"<p><p>Restrictive fluid management (RFM) for hemodynamically unstable trauma patients has reduced mortality rates. The objective was to determine whether RFM benefits geriatric hip fracture patients, who are usually hemodynamically stable.</p><p><strong>Design: </strong>Retrospective propensity-matched study.</p><p><strong>Setting: </strong>Five Level I trauma centers (January 1, 2018-December 12, 2018).</p><p><strong>Patients: </strong>Geriatric patients (65 years or older) with hip fractures were included in this study. Patients with multiple injuries, nonoperative management, and preoperative blood products were excluded.</p><p><strong>Intervention: </strong>Patients were grouped by fluid volume (normal saline, lactated Ringer, dextrose, electrolytes, and medications) received preoperatively or ≤24 hours of arrival; patients with standard fluid management (SFM) received ≥150 mL and RFM <150 mL of fluids.</p><p><strong>Main outcome measurements: </strong>The primary outcomes were length of stay (LOS), delayed ambulation (>2 days postoperatively), and mortality. Paired Student t-tests, Wilcoxon paired rank sum tests, and McNemar tests were used; an α value of < 0.05 was considered statistically significant.</p><p><strong>Results: </strong>There were 523 patients (40% RFM, 60% SFM); after matching, there were 95 patients per arm. The matched patients were well-balanced, including no difference in time from arrival to surgery. RFM and SFM patients received a median of 80 mL and 1250 mL of preoperative fluids, respectively (<i>P</i> < 0.001). Postoperative fluid volumes were 1550 versus 2000 mL, respectively, (<i>P</i> = 0.73), and LOSs were similar between the two groups (5 versus 5 days, <i>P</i> = 0.83). Mortality and complications, including acute kidney injuries, were similar. Delayed ambulation rates were similar overall. When stratified by preinjury ambulation status, SFM was associated with delayed ambulation for patients not walking independently before injury (<i>P</i> = 0.01), but RFM was not (<i>P</i> = 0.09).</p><p><strong>Conclusions: </strong>RFM seems to be safe in terms of laboratory results, complications, and disposition. SFM may lead to delayed ambulation for patients who are not walking independently before injury.</p>","PeriodicalId":74381,"journal":{"name":"OTA international : the open access journal of orthopaedic trauma","volume":"6 3","pages":"e279"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/87/01/oi9-6-e279.PMC10356122.pdf","citationCount":"0","resultStr":"{\"title\":\"The effect of restrictive fluid management on outcomes among geriatric hip fractures: a retrospective cohort study at five level I trauma centers.\",\"authors\":\"Jordan Willis, Stephanie Jarvis, Gina M Berg, Chad Corrigan, Robert Madayag, Cassandra Reynolds, Allen Tanner, Gary Marshall, Carlos Palacio Lascano, David Bar-Or\",\"doi\":\"10.1097/OI9.0000000000000279\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Restrictive fluid management (RFM) for hemodynamically unstable trauma patients has reduced mortality rates. The objective was to determine whether RFM benefits geriatric hip fracture patients, who are usually hemodynamically stable.</p><p><strong>Design: </strong>Retrospective propensity-matched study.</p><p><strong>Setting: </strong>Five Level I trauma centers (January 1, 2018-December 12, 2018).</p><p><strong>Patients: </strong>Geriatric patients (65 years or older) with hip fractures were included in this study. Patients with multiple injuries, nonoperative management, and preoperative blood products were excluded.</p><p><strong>Intervention: </strong>Patients were grouped by fluid volume (normal saline, lactated Ringer, dextrose, electrolytes, and medications) received preoperatively or ≤24 hours of arrival; patients with standard fluid management (SFM) received ≥150 mL and RFM <150 mL of fluids.</p><p><strong>Main outcome measurements: </strong>The primary outcomes were length of stay (LOS), delayed ambulation (>2 days postoperatively), and mortality. Paired Student t-tests, Wilcoxon paired rank sum tests, and McNemar tests were used; an α value of < 0.05 was considered statistically significant.</p><p><strong>Results: </strong>There were 523 patients (40% RFM, 60% SFM); after matching, there were 95 patients per arm. The matched patients were well-balanced, including no difference in time from arrival to surgery. RFM and SFM patients received a median of 80 mL and 1250 mL of preoperative fluids, respectively (<i>P</i> < 0.001). Postoperative fluid volumes were 1550 versus 2000 mL, respectively, (<i>P</i> = 0.73), and LOSs were similar between the two groups (5 versus 5 days, <i>P</i> = 0.83). Mortality and complications, including acute kidney injuries, were similar. Delayed ambulation rates were similar overall. When stratified by preinjury ambulation status, SFM was associated with delayed ambulation for patients not walking independently before injury (<i>P</i> = 0.01), but RFM was not (<i>P</i> = 0.09).</p><p><strong>Conclusions: </strong>RFM seems to be safe in terms of laboratory results, complications, and disposition. SFM may lead to delayed ambulation for patients who are not walking independently before injury.</p>\",\"PeriodicalId\":74381,\"journal\":{\"name\":\"OTA international : the open access journal of orthopaedic trauma\",\"volume\":\"6 3\",\"pages\":\"e279\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/87/01/oi9-6-e279.PMC10356122.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"OTA international : the open access journal of orthopaedic trauma\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/OI9.0000000000000279\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"OTA international : the open access journal of orthopaedic trauma","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/OI9.0000000000000279","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
The effect of restrictive fluid management on outcomes among geriatric hip fractures: a retrospective cohort study at five level I trauma centers.
Restrictive fluid management (RFM) for hemodynamically unstable trauma patients has reduced mortality rates. The objective was to determine whether RFM benefits geriatric hip fracture patients, who are usually hemodynamically stable.
Design: Retrospective propensity-matched study.
Setting: Five Level I trauma centers (January 1, 2018-December 12, 2018).
Patients: Geriatric patients (65 years or older) with hip fractures were included in this study. Patients with multiple injuries, nonoperative management, and preoperative blood products were excluded.
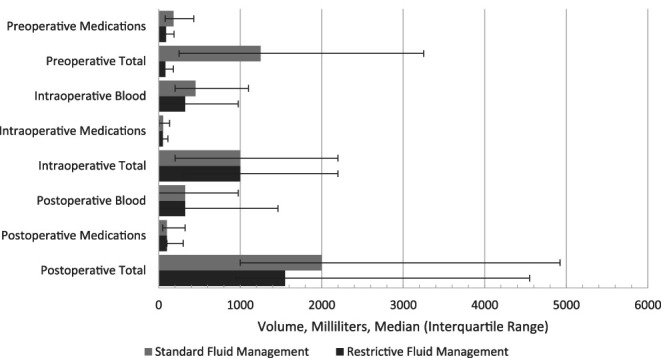
Intervention: Patients were grouped by fluid volume (normal saline, lactated Ringer, dextrose, electrolytes, and medications) received preoperatively or ≤24 hours of arrival; patients with standard fluid management (SFM) received ≥150 mL and RFM <150 mL of fluids.
Main outcome measurements: The primary outcomes were length of stay (LOS), delayed ambulation (>2 days postoperatively), and mortality. Paired Student t-tests, Wilcoxon paired rank sum tests, and McNemar tests were used; an α value of < 0.05 was considered statistically significant.
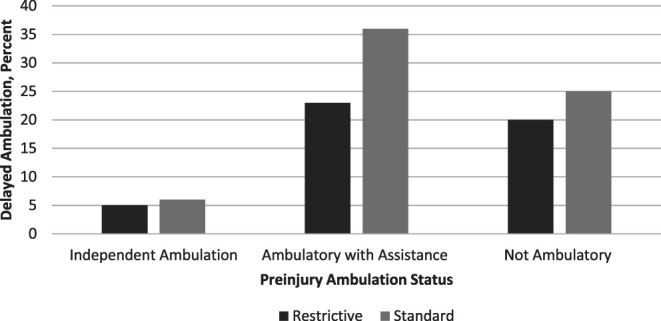
Results: There were 523 patients (40% RFM, 60% SFM); after matching, there were 95 patients per arm. The matched patients were well-balanced, including no difference in time from arrival to surgery. RFM and SFM patients received a median of 80 mL and 1250 mL of preoperative fluids, respectively (P < 0.001). Postoperative fluid volumes were 1550 versus 2000 mL, respectively, (P = 0.73), and LOSs were similar between the two groups (5 versus 5 days, P = 0.83). Mortality and complications, including acute kidney injuries, were similar. Delayed ambulation rates were similar overall. When stratified by preinjury ambulation status, SFM was associated with delayed ambulation for patients not walking independently before injury (P = 0.01), but RFM was not (P = 0.09).
Conclusions: RFM seems to be safe in terms of laboratory results, complications, and disposition. SFM may lead to delayed ambulation for patients who are not walking independently before injury.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


