Shelley Brukman, Makenzie J Ferguson, Kimberly D Zaky, Chloe Knudsen-Robbins, Theodore W Heyming
{"title":"儿童虐待教育:利用密室逃生活动吸引学习者对一个敏感的话题。","authors":"Shelley Brukman, Makenzie J Ferguson, Kimberly D Zaky, Chloe Knudsen-Robbins, Theodore W Heyming","doi":"10.21980/J84H1C","DOIUrl":null,"url":null,"abstract":"<p><strong>Audience: </strong>Emergency medical service (EMS) providers and other health care professionals.</p><p><strong>Introduction: </strong>In 2019 alone, 656,000 children in the United States were victims of child abuse and neglect.1 The medical community has historically struggled with the identification of child maltreatment. In one study, 33% of abused children had a previous visit with a medical provider in which the abuse was found to have been missed.2 Many voices in the healthcare community have advocated for the implementation of routine screening, and studies have demonstrated the implementation of such screening in the emergency department (ED) increases the detection of child maltreatment.3-7 Child maltreatment screening tools are increasingly utilized in primary care and ED settings, but one has yet to be adapted or designed for universal use by emergency medical services (EMS) professionals in the prehospital care context. Because EMS providers are uniquely positioned to assess for maltreatment, they have traditionally been the only provider to interact with families in the home environment. Unfortunately, EMS rates of documentation of maltreatment is quite low. A recent study using the National Emergency Medical Services Information System database to evaluate EMS documentation of child maltreatment in patients ≤3 years of age compared to the national incidence of known maltreatment found an almost 15-fold discrepancy.8 There have been several attempts to elucidate the difficulties of and barriers to reporting by EMS providers. Markenson et al and Tiyyagura et al outlined several areas that potentially contribute to a lack of reporting: minimal continuing medical education (CME) on child maltreatment, knowledge of physical and historical details suspicious for abuse, knowledge of child development, limited clinical evaluation time in a fast-paced work environment, understanding of how to appropriately interact with families, and fear of being wrong.9,10 This class/escape room activity was developed to directly address several of these areas. Emergency medical service providers participate in traditional didactics (in the form of a short lecture), followed by an escape room activity in which they further explore and reinforce learning in a fun and memorable environment. This activity also promotes teamwork, an especially important skill in potentially complex and difficult situations such as those surrounding suspected child maltreatment.</p><p><strong>Educational objectives: </strong>By the end of the escape room, the learner should be able to: 1) understand the national and local prevalence of child maltreatment; 2) understand the different types of child maltreatment and common associated presentations; 3) know the local EMS agency reporting requirements; 4) understand when to make base hospital contact with respect to concern for maltreatment; 5) collaborate effectively as a team.</p><p><strong>Educational methods: </strong>Child maltreatment can be a sensitive and challenging topic. In this class, we presented learners with a short, 15-minute lecture (see Pre-Escape Room Lecture PowerPoint) followed by an escape room activity. The Pre-Escape Room Lecture PowerPoint includes suggestions on the type of image and/or statistics to include on each slide, which can be taken from your site's available de-identified photos and information. The lecture included material describing national and local statistics on child maltreatment, definitions of abuse, and techniques to help identify concern for maltreatment. Learners were free to ask questions following lecture. They were then divided into their assigned crews/teams for the escape room activity. The puzzles in the escape room served to reinforce concepts and details presented in lecture. We held a debrief after the escape room activity to discuss puzzle answers and address any follow-up questions.</p><p><strong>Research methods: </strong>Learners completed a program evaluation after the activity. These questions assessed the learners' perception of the importance and applicability of the content presented, the escape room format, and what they felt was the most significant and helpful to their practice.</p><p><strong>Results: </strong>Learners reported enjoying the activity and felt the escape room-based approach allowed for deeper engagement with the topic since the serious nature of child maltreatment can sometimes make this difficult.</p><p><strong>Discussion: </strong>Pediatric abuse and neglect is a serious and often heavy topic to present to healthcare providers. While we took into consideration that presenting a sensitive topic such as child abuse in an escape room format may be perceived as insensitive or display a lack of insight or respect for the topic, we also understood that the way we built out the clues and puzzles would be important in how the game was perceived by the participants. By building the puzzles to be factual and not overly excessive, we allowed the learners to interact with the information and practice identifying possible cases of abuse and how and when to report suspicions in a manner that did not trivialize the seriousness of the topic or take away from the fact that they were competing in a game. We used a PowerPoint lecture to present the foundation of the content and then lightened the learning session with the use of the escape room activity. The level of competition and comradery lightened the overall mood, and the learners left the class on a high note.</p><p><strong>Topics: </strong>Child abuse recognition, escape room activity, small-group activity, prehospital, neglect, physical abuse, emotional abuse, sexual abuse, mandated reporter.</p>","PeriodicalId":73721,"journal":{"name":"Journal of education & teaching in emergency medicine","volume":"8 1","pages":"SG1-SG21"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10332768/pdf/","citationCount":"0","resultStr":"{\"title\":\"Child Maltreatment Education: Utilizing an Escape Room Activity to Engage Learners on a Sensitive Topic.\",\"authors\":\"Shelley Brukman, Makenzie J Ferguson, Kimberly D Zaky, Chloe Knudsen-Robbins, Theodore W Heyming\",\"doi\":\"10.21980/J84H1C\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Audience: </strong>Emergency medical service (EMS) providers and other health care professionals.</p><p><strong>Introduction: </strong>In 2019 alone, 656,000 children in the United States were victims of child abuse and neglect.1 The medical community has historically struggled with the identification of child maltreatment. In one study, 33% of abused children had a previous visit with a medical provider in which the abuse was found to have been missed.2 Many voices in the healthcare community have advocated for the implementation of routine screening, and studies have demonstrated the implementation of such screening in the emergency department (ED) increases the detection of child maltreatment.3-7 Child maltreatment screening tools are increasingly utilized in primary care and ED settings, but one has yet to be adapted or designed for universal use by emergency medical services (EMS) professionals in the prehospital care context. Because EMS providers are uniquely positioned to assess for maltreatment, they have traditionally been the only provider to interact with families in the home environment. Unfortunately, EMS rates of documentation of maltreatment is quite low. A recent study using the National Emergency Medical Services Information System database to evaluate EMS documentation of child maltreatment in patients ≤3 years of age compared to the national incidence of known maltreatment found an almost 15-fold discrepancy.8 There have been several attempts to elucidate the difficulties of and barriers to reporting by EMS providers. Markenson et al and Tiyyagura et al outlined several areas that potentially contribute to a lack of reporting: minimal continuing medical education (CME) on child maltreatment, knowledge of physical and historical details suspicious for abuse, knowledge of child development, limited clinical evaluation time in a fast-paced work environment, understanding of how to appropriately interact with families, and fear of being wrong.9,10 This class/escape room activity was developed to directly address several of these areas. Emergency medical service providers participate in traditional didactics (in the form of a short lecture), followed by an escape room activity in which they further explore and reinforce learning in a fun and memorable environment. This activity also promotes teamwork, an especially important skill in potentially complex and difficult situations such as those surrounding suspected child maltreatment.</p><p><strong>Educational objectives: </strong>By the end of the escape room, the learner should be able to: 1) understand the national and local prevalence of child maltreatment; 2) understand the different types of child maltreatment and common associated presentations; 3) know the local EMS agency reporting requirements; 4) understand when to make base hospital contact with respect to concern for maltreatment; 5) collaborate effectively as a team.</p><p><strong>Educational methods: </strong>Child maltreatment can be a sensitive and challenging topic. In this class, we presented learners with a short, 15-minute lecture (see Pre-Escape Room Lecture PowerPoint) followed by an escape room activity. The Pre-Escape Room Lecture PowerPoint includes suggestions on the type of image and/or statistics to include on each slide, which can be taken from your site's available de-identified photos and information. The lecture included material describing national and local statistics on child maltreatment, definitions of abuse, and techniques to help identify concern for maltreatment. Learners were free to ask questions following lecture. They were then divided into their assigned crews/teams for the escape room activity. The puzzles in the escape room served to reinforce concepts and details presented in lecture. We held a debrief after the escape room activity to discuss puzzle answers and address any follow-up questions.</p><p><strong>Research methods: </strong>Learners completed a program evaluation after the activity. These questions assessed the learners' perception of the importance and applicability of the content presented, the escape room format, and what they felt was the most significant and helpful to their practice.</p><p><strong>Results: </strong>Learners reported enjoying the activity and felt the escape room-based approach allowed for deeper engagement with the topic since the serious nature of child maltreatment can sometimes make this difficult.</p><p><strong>Discussion: </strong>Pediatric abuse and neglect is a serious and often heavy topic to present to healthcare providers. While we took into consideration that presenting a sensitive topic such as child abuse in an escape room format may be perceived as insensitive or display a lack of insight or respect for the topic, we also understood that the way we built out the clues and puzzles would be important in how the game was perceived by the participants. By building the puzzles to be factual and not overly excessive, we allowed the learners to interact with the information and practice identifying possible cases of abuse and how and when to report suspicions in a manner that did not trivialize the seriousness of the topic or take away from the fact that they were competing in a game. We used a PowerPoint lecture to present the foundation of the content and then lightened the learning session with the use of the escape room activity. The level of competition and comradery lightened the overall mood, and the learners left the class on a high note.</p><p><strong>Topics: </strong>Child abuse recognition, escape room activity, small-group activity, prehospital, neglect, physical abuse, emotional abuse, sexual abuse, mandated reporter.</p>\",\"PeriodicalId\":73721,\"journal\":{\"name\":\"Journal of education & teaching in emergency medicine\",\"volume\":\"8 1\",\"pages\":\"SG1-SG21\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10332768/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of education & teaching in emergency medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21980/J84H1C\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of education & teaching in emergency medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21980/J84H1C","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Child Maltreatment Education: Utilizing an Escape Room Activity to Engage Learners on a Sensitive Topic.
Audience: Emergency medical service (EMS) providers and other health care professionals.
Introduction: In 2019 alone, 656,000 children in the United States were victims of child abuse and neglect.1 The medical community has historically struggled with the identification of child maltreatment. In one study, 33% of abused children had a previous visit with a medical provider in which the abuse was found to have been missed.2 Many voices in the healthcare community have advocated for the implementation of routine screening, and studies have demonstrated the implementation of such screening in the emergency department (ED) increases the detection of child maltreatment.3-7 Child maltreatment screening tools are increasingly utilized in primary care and ED settings, but one has yet to be adapted or designed for universal use by emergency medical services (EMS) professionals in the prehospital care context. Because EMS providers are uniquely positioned to assess for maltreatment, they have traditionally been the only provider to interact with families in the home environment. Unfortunately, EMS rates of documentation of maltreatment is quite low. A recent study using the National Emergency Medical Services Information System database to evaluate EMS documentation of child maltreatment in patients ≤3 years of age compared to the national incidence of known maltreatment found an almost 15-fold discrepancy.8 There have been several attempts to elucidate the difficulties of and barriers to reporting by EMS providers. Markenson et al and Tiyyagura et al outlined several areas that potentially contribute to a lack of reporting: minimal continuing medical education (CME) on child maltreatment, knowledge of physical and historical details suspicious for abuse, knowledge of child development, limited clinical evaluation time in a fast-paced work environment, understanding of how to appropriately interact with families, and fear of being wrong.9,10 This class/escape room activity was developed to directly address several of these areas. Emergency medical service providers participate in traditional didactics (in the form of a short lecture), followed by an escape room activity in which they further explore and reinforce learning in a fun and memorable environment. This activity also promotes teamwork, an especially important skill in potentially complex and difficult situations such as those surrounding suspected child maltreatment.
Educational objectives: By the end of the escape room, the learner should be able to: 1) understand the national and local prevalence of child maltreatment; 2) understand the different types of child maltreatment and common associated presentations; 3) know the local EMS agency reporting requirements; 4) understand when to make base hospital contact with respect to concern for maltreatment; 5) collaborate effectively as a team.
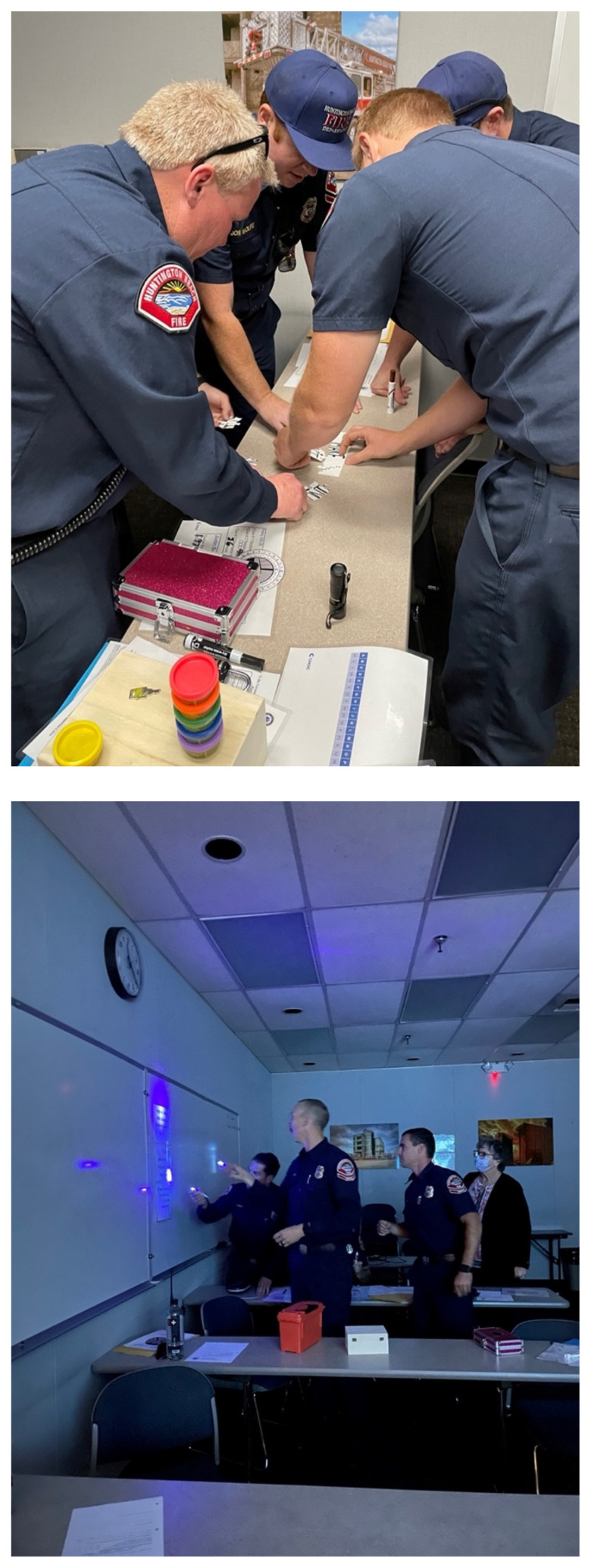
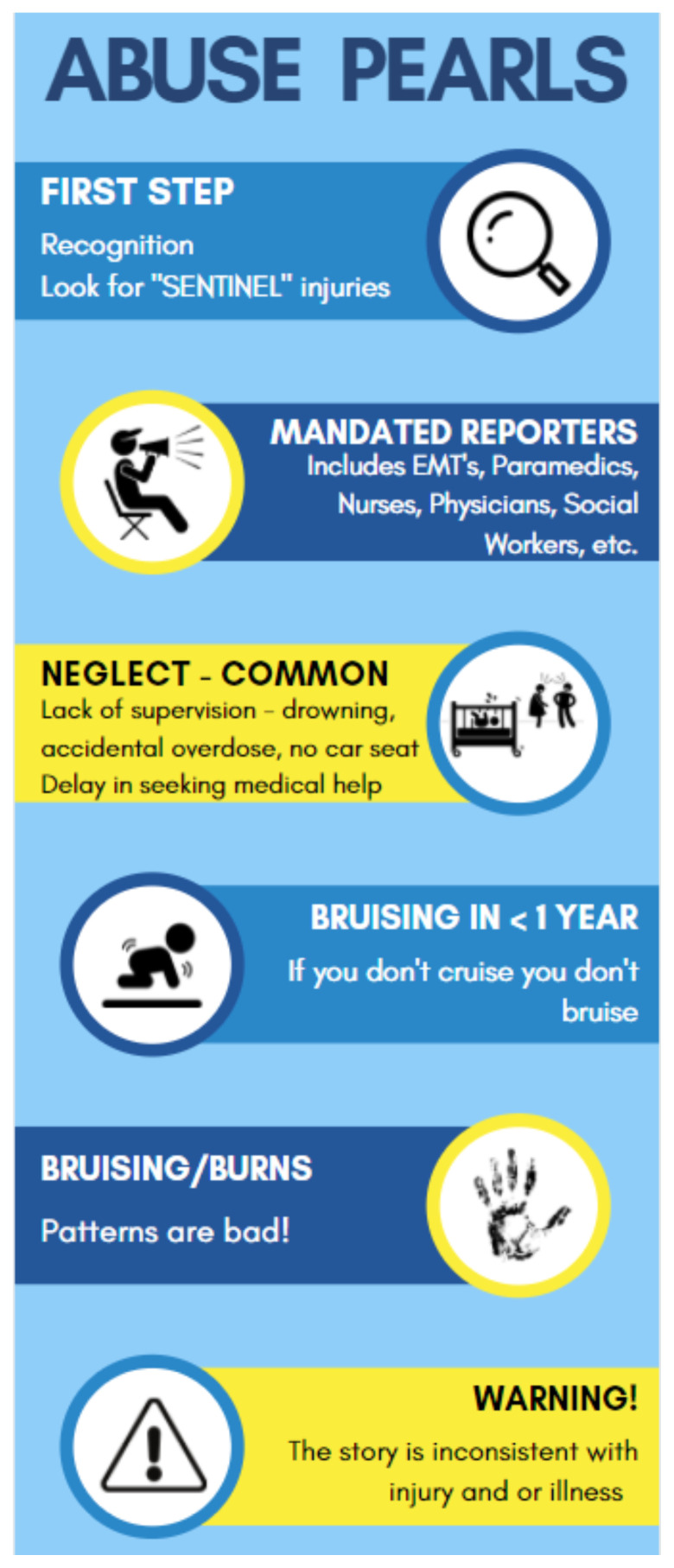
Educational methods: Child maltreatment can be a sensitive and challenging topic. In this class, we presented learners with a short, 15-minute lecture (see Pre-Escape Room Lecture PowerPoint) followed by an escape room activity. The Pre-Escape Room Lecture PowerPoint includes suggestions on the type of image and/or statistics to include on each slide, which can be taken from your site's available de-identified photos and information. The lecture included material describing national and local statistics on child maltreatment, definitions of abuse, and techniques to help identify concern for maltreatment. Learners were free to ask questions following lecture. They were then divided into their assigned crews/teams for the escape room activity. The puzzles in the escape room served to reinforce concepts and details presented in lecture. We held a debrief after the escape room activity to discuss puzzle answers and address any follow-up questions.
Research methods: Learners completed a program evaluation after the activity. These questions assessed the learners' perception of the importance and applicability of the content presented, the escape room format, and what they felt was the most significant and helpful to their practice.
Results: Learners reported enjoying the activity and felt the escape room-based approach allowed for deeper engagement with the topic since the serious nature of child maltreatment can sometimes make this difficult.
Discussion: Pediatric abuse and neglect is a serious and often heavy topic to present to healthcare providers. While we took into consideration that presenting a sensitive topic such as child abuse in an escape room format may be perceived as insensitive or display a lack of insight or respect for the topic, we also understood that the way we built out the clues and puzzles would be important in how the game was perceived by the participants. By building the puzzles to be factual and not overly excessive, we allowed the learners to interact with the information and practice identifying possible cases of abuse and how and when to report suspicions in a manner that did not trivialize the seriousness of the topic or take away from the fact that they were competing in a game. We used a PowerPoint lecture to present the foundation of the content and then lightened the learning session with the use of the escape room activity. The level of competition and comradery lightened the overall mood, and the learners left the class on a high note.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


