Shea Polancich, Patricia Patrician, Rebecca Miltner, Katherine Meese, Amy Armstrong, Shannon Layton, Ross Vander Noot, Terri Poe, Allyson G. Hall
{"title":"在学习型健康中心减少医院获得性压力伤害:为质量辩护","authors":"Shea Polancich, Patricia Patrician, Rebecca Miltner, Katherine Meese, Amy Armstrong, Shannon Layton, Ross Vander Noot, Terri Poe, Allyson G. Hall","doi":"10.1002/lrh2.10355","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>The purpose of this descriptive study is to examine a learning health system (LHS) continuous improvement and learning approach as a case for increased quality, standardized processes, redesigned workflows, and better resource utilization. Hospital acquired pressure injuries (HAPI) commonly occur in the hospitalized patient and are costly and preventable. This study examines the effect of a LHS approach to reducing HAPI within a large academic medical center.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Our learning health center implemented a 6-year series of iterative improvements that included both process and technology changes, with robust data and analytical reforms. In this descriptive, observational study, we retrospectively examined longitudinal data from April 1, 2018 to March 31, 2022, examining the variables of total number of all-stage HAPI counts and average length of stay (ALOS). We also analyzed patient characteristics observed/expected mortality ratios, as well as total patient days, and the case-mix index to determine whether these factors varied over the study period. We used the Agency for Healthcare Research and Quality cost estimates to identify the estimated financial benefit of HAPI reductions on an annualized basis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>HAPI per 1000 patient days for FY 20 (October 1-September 30) and FY 21, decreased from 2.30 to 1.30 and annualized event AHRQ cost estimates for HAPI decreased by $4 786 980 from FY 20 to FY 21. A strong, statistically significant, negative and seemingly counterintuitive correlation was found (<i>r</i> = −.524, <i>P</i> = .003) between HAPI and ALOS.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>The LHS efforts directed toward HAPI reduction led to sustained improvements during the study period. These results demonstrate the benefits of a holistic approach to quality improvement offered by the LHS model. The LHS model goes beyond a problem-based approach to process improvement. Rather than targeting a specific problem to solve, the LHS system creates structures that yield process improvement benefits over a continued time period.</p>\n </section>\n </div>","PeriodicalId":43916,"journal":{"name":"Learning Health Systems","volume":"7 3","pages":""},"PeriodicalIF":2.6000,"publicationDate":"2022-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lrh2.10355","citationCount":"1","resultStr":"{\"title\":\"Reducing hospital acquired pressure injury in a learning health center: Making the case for quality\",\"authors\":\"Shea Polancich, Patricia Patrician, Rebecca Miltner, Katherine Meese, Amy Armstrong, Shannon Layton, Ross Vander Noot, Terri Poe, Allyson G. Hall\",\"doi\":\"10.1002/lrh2.10355\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>The purpose of this descriptive study is to examine a learning health system (LHS) continuous improvement and learning approach as a case for increased quality, standardized processes, redesigned workflows, and better resource utilization. Hospital acquired pressure injuries (HAPI) commonly occur in the hospitalized patient and are costly and preventable. This study examines the effect of a LHS approach to reducing HAPI within a large academic medical center.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Our learning health center implemented a 6-year series of iterative improvements that included both process and technology changes, with robust data and analytical reforms. In this descriptive, observational study, we retrospectively examined longitudinal data from April 1, 2018 to March 31, 2022, examining the variables of total number of all-stage HAPI counts and average length of stay (ALOS). We also analyzed patient characteristics observed/expected mortality ratios, as well as total patient days, and the case-mix index to determine whether these factors varied over the study period. We used the Agency for Healthcare Research and Quality cost estimates to identify the estimated financial benefit of HAPI reductions on an annualized basis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>HAPI per 1000 patient days for FY 20 (October 1-September 30) and FY 21, decreased from 2.30 to 1.30 and annualized event AHRQ cost estimates for HAPI decreased by $4 786 980 from FY 20 to FY 21. A strong, statistically significant, negative and seemingly counterintuitive correlation was found (<i>r</i> = −.524, <i>P</i> = .003) between HAPI and ALOS.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>The LHS efforts directed toward HAPI reduction led to sustained improvements during the study period. These results demonstrate the benefits of a holistic approach to quality improvement offered by the LHS model. The LHS model goes beyond a problem-based approach to process improvement. Rather than targeting a specific problem to solve, the LHS system creates structures that yield process improvement benefits over a continued time period.</p>\\n </section>\\n </div>\",\"PeriodicalId\":43916,\"journal\":{\"name\":\"Learning Health Systems\",\"volume\":\"7 3\",\"pages\":\"\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2022-12-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lrh2.10355\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Learning Health Systems\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/lrh2.10355\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Learning Health Systems","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lrh2.10355","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
Reducing hospital acquired pressure injury in a learning health center: Making the case for quality
Introduction
The purpose of this descriptive study is to examine a learning health system (LHS) continuous improvement and learning approach as a case for increased quality, standardized processes, redesigned workflows, and better resource utilization. Hospital acquired pressure injuries (HAPI) commonly occur in the hospitalized patient and are costly and preventable. This study examines the effect of a LHS approach to reducing HAPI within a large academic medical center.
Methods
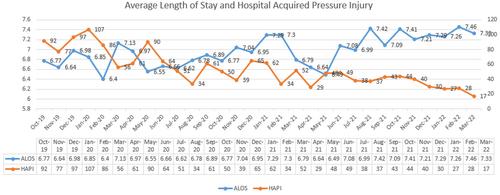
Our learning health center implemented a 6-year series of iterative improvements that included both process and technology changes, with robust data and analytical reforms. In this descriptive, observational study, we retrospectively examined longitudinal data from April 1, 2018 to March 31, 2022, examining the variables of total number of all-stage HAPI counts and average length of stay (ALOS). We also analyzed patient characteristics observed/expected mortality ratios, as well as total patient days, and the case-mix index to determine whether these factors varied over the study period. We used the Agency for Healthcare Research and Quality cost estimates to identify the estimated financial benefit of HAPI reductions on an annualized basis.
Results
HAPI per 1000 patient days for FY 20 (October 1-September 30) and FY 21, decreased from 2.30 to 1.30 and annualized event AHRQ cost estimates for HAPI decreased by $4 786 980 from FY 20 to FY 21. A strong, statistically significant, negative and seemingly counterintuitive correlation was found (r = −.524, P = .003) between HAPI and ALOS.
Conclusions
The LHS efforts directed toward HAPI reduction led to sustained improvements during the study period. These results demonstrate the benefits of a holistic approach to quality improvement offered by the LHS model. The LHS model goes beyond a problem-based approach to process improvement. Rather than targeting a specific problem to solve, the LHS system creates structures that yield process improvement benefits over a continued time period.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


