Stephen S Johnston, Mosadoluwa Afolabi, Pranjal Tewari, Walter Danker
{"title":"与破坏性手术出血相关的临床和经济负担:回顾性数据库分析。","authors":"Stephen S Johnston, Mosadoluwa Afolabi, Pranjal Tewari, Walter Danker","doi":"10.2147/CEOR.S411778","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hemostatic agents are used to control surgical bleeding; however, some patients experience disruptive bleeding despite the use of hemostats. In patients receiving hemostats, we compared clinical and economic outcomes between patients with vs without disruptive bleeding during a variety of surgical procedures.</p><p><strong>Methods: </strong>This was a retrospective analysis of the Premier Healthcare Database. Study patients were age ≥18 with a hospital encounter for one of 9 procedures with evidence of hemostatic agent use between 1-Jan-2019 and 31-Dec-2019: cholecystectomy, coronary artery bypass grafting (CABG), cystectomy, hepatectomy, hysterectomy, pancreatectomy, peripheral vascular, thoracic, and valve procedures (first procedure = index). Patients were grouped by presence vs absence of disruptive bleeding. Outcomes evaluated during index included intensive care unit (ICU) admission/duration, ventilator use, operating room time, length of stay (LOS), in-hospital mortality, and total hospital costs; 90-day all-cause inpatient readmission was also evaluated. Multivariable analyses were used to examine the association of disruptive bleeding with outcomes, adjusting for patient, procedure, and hospital/provider characteristics.</p><p><strong>Results: </strong>The study included 51,448 patients; 16% had disruptive bleeding (range 1.5% for cholecystectomy to 44.4% for valve). In procedures for which ICU and ventilator use is not routine, disruptive bleeding was associated with significant increases in the risks of admission to ICU and requirement for ventilator (all p≤0.05). Across all procedures, disruptive bleeding was also associated with significant incremental increases in days spent in ICU (all p≤0.05, except CABG), LOS (all p≤0.05, except thoracic), and total hospital costs (all p≤0.05); 90-day all-cause inpatient readmission, in-hospital mortality, and operating room time were higher in the presence of disruptive bleeding and varied in statistical significance across procedures.</p><p><strong>Conclusion: </strong>Disruptive bleeding was associated with substantial clinical and economic burden across a wide variety of surgical procedures. Findings emphasize the need for more effective and timely intervention for surgical bleeding events.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"15 ","pages":"535-547"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4b/09/ceor-15-535.PMC10327677.pdf","citationCount":"0","resultStr":"{\"title\":\"Clinical and Economic Burden Associated with Disruptive Surgical Bleeding: A Retrospective Database Analysis.\",\"authors\":\"Stephen S Johnston, Mosadoluwa Afolabi, Pranjal Tewari, Walter Danker\",\"doi\":\"10.2147/CEOR.S411778\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hemostatic agents are used to control surgical bleeding; however, some patients experience disruptive bleeding despite the use of hemostats. In patients receiving hemostats, we compared clinical and economic outcomes between patients with vs without disruptive bleeding during a variety of surgical procedures.</p><p><strong>Methods: </strong>This was a retrospective analysis of the Premier Healthcare Database. Study patients were age ≥18 with a hospital encounter for one of 9 procedures with evidence of hemostatic agent use between 1-Jan-2019 and 31-Dec-2019: cholecystectomy, coronary artery bypass grafting (CABG), cystectomy, hepatectomy, hysterectomy, pancreatectomy, peripheral vascular, thoracic, and valve procedures (first procedure = index). Patients were grouped by presence vs absence of disruptive bleeding. Outcomes evaluated during index included intensive care unit (ICU) admission/duration, ventilator use, operating room time, length of stay (LOS), in-hospital mortality, and total hospital costs; 90-day all-cause inpatient readmission was also evaluated. Multivariable analyses were used to examine the association of disruptive bleeding with outcomes, adjusting for patient, procedure, and hospital/provider characteristics.</p><p><strong>Results: </strong>The study included 51,448 patients; 16% had disruptive bleeding (range 1.5% for cholecystectomy to 44.4% for valve). In procedures for which ICU and ventilator use is not routine, disruptive bleeding was associated with significant increases in the risks of admission to ICU and requirement for ventilator (all p≤0.05). Across all procedures, disruptive bleeding was also associated with significant incremental increases in days spent in ICU (all p≤0.05, except CABG), LOS (all p≤0.05, except thoracic), and total hospital costs (all p≤0.05); 90-day all-cause inpatient readmission, in-hospital mortality, and operating room time were higher in the presence of disruptive bleeding and varied in statistical significance across procedures.</p><p><strong>Conclusion: </strong>Disruptive bleeding was associated with substantial clinical and economic burden across a wide variety of surgical procedures. Findings emphasize the need for more effective and timely intervention for surgical bleeding events.</p>\",\"PeriodicalId\":47313,\"journal\":{\"name\":\"ClinicoEconomics and Outcomes Research\",\"volume\":\"15 \",\"pages\":\"535-547\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4b/09/ceor-15-535.PMC10327677.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ClinicoEconomics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEOR.S411778\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S411778","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Clinical and Economic Burden Associated with Disruptive Surgical Bleeding: A Retrospective Database Analysis.
Background: Hemostatic agents are used to control surgical bleeding; however, some patients experience disruptive bleeding despite the use of hemostats. In patients receiving hemostats, we compared clinical and economic outcomes between patients with vs without disruptive bleeding during a variety of surgical procedures.
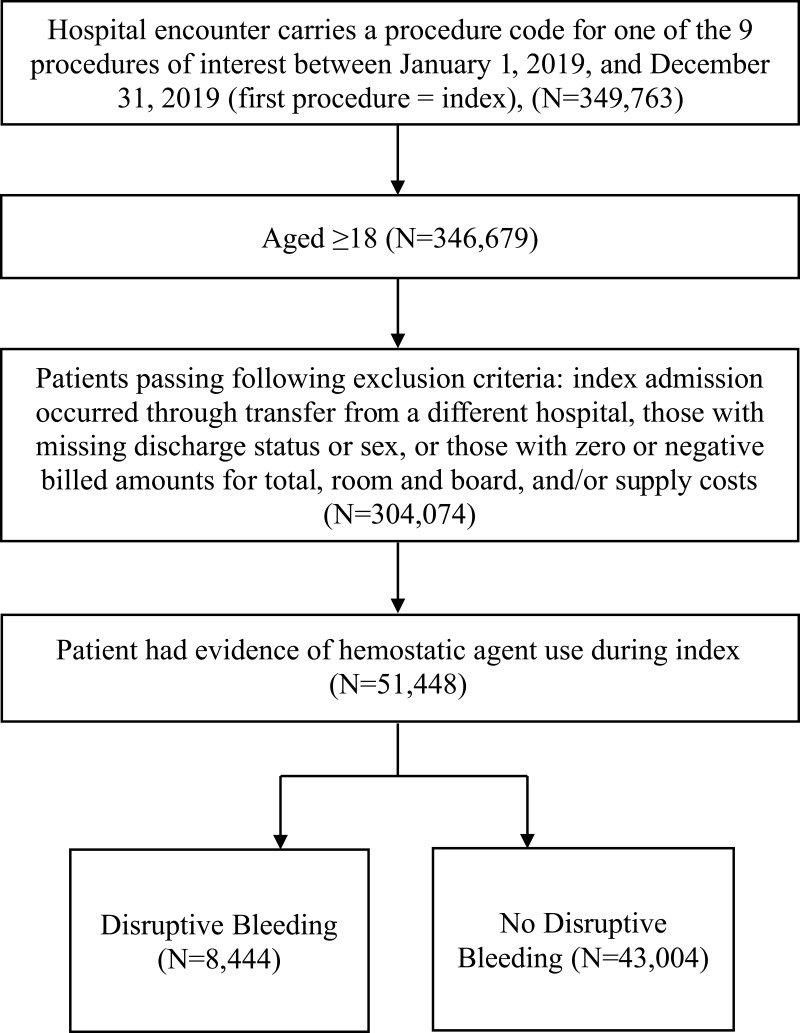
Methods: This was a retrospective analysis of the Premier Healthcare Database. Study patients were age ≥18 with a hospital encounter for one of 9 procedures with evidence of hemostatic agent use between 1-Jan-2019 and 31-Dec-2019: cholecystectomy, coronary artery bypass grafting (CABG), cystectomy, hepatectomy, hysterectomy, pancreatectomy, peripheral vascular, thoracic, and valve procedures (first procedure = index). Patients were grouped by presence vs absence of disruptive bleeding. Outcomes evaluated during index included intensive care unit (ICU) admission/duration, ventilator use, operating room time, length of stay (LOS), in-hospital mortality, and total hospital costs; 90-day all-cause inpatient readmission was also evaluated. Multivariable analyses were used to examine the association of disruptive bleeding with outcomes, adjusting for patient, procedure, and hospital/provider characteristics.
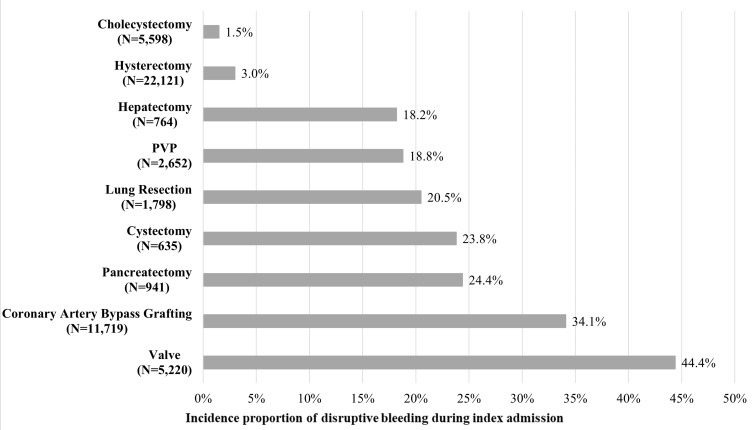
Results: The study included 51,448 patients; 16% had disruptive bleeding (range 1.5% for cholecystectomy to 44.4% for valve). In procedures for which ICU and ventilator use is not routine, disruptive bleeding was associated with significant increases in the risks of admission to ICU and requirement for ventilator (all p≤0.05). Across all procedures, disruptive bleeding was also associated with significant incremental increases in days spent in ICU (all p≤0.05, except CABG), LOS (all p≤0.05, except thoracic), and total hospital costs (all p≤0.05); 90-day all-cause inpatient readmission, in-hospital mortality, and operating room time were higher in the presence of disruptive bleeding and varied in statistical significance across procedures.
Conclusion: Disruptive bleeding was associated with substantial clinical and economic burden across a wide variety of surgical procedures. Findings emphasize the need for more effective and timely intervention for surgical bleeding events.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


