Diane M Harper, Rye J Anderson, Ed Baker, Tiffany M Yu
{"title":"用于宫颈癌筛查的 hrHPV 基因分型联合检测后 p16/Ki-67 双染色细胞学反射的成本效益。","authors":"Diane M Harper, Rye J Anderson, Ed Baker, Tiffany M Yu","doi":"10.1158/1940-6207.CAPR-22-0455","DOIUrl":null,"url":null,"abstract":"<p><p>The first biomarker-based cervical cancer screening test, p16/Ki-67 dual-stained cytology (DS), has been clinically validated and approved in the United States for triage of women being screened for cervical cancer who test positive for high-risk human papillomavirus (hrHPV). The primary aim of this work is to evaluate the cost-effectiveness of DS triage after co-testing findings of positive non-16/18 HPV types and atypical squamous cells of undetermined significance or low-grade squamous intraepithelial lesions cytology. A payer-perspective Markov microsimulation model was developed to assess the impact of DS reflex testing. Each comparison simulated 12,250 screening-eligible women through health states defined by hrHPV status and genotype, cervical intraepithelial neoplasia grades 1-3, invasive cervical cancer (ICC) by stage, and cancer-related or non-cancer death. Screening test performance data were from the IMPACT clinical validation trial. Transition probabilities were from population and natural history studies. Costs of baseline medical care, screening visits, tests, procedures, and ICC were included. DS reflex after co-testing was cost-effective with incremental cost-effectiveness ratios per quality-adjusted life-year gained of $15,231 [95% confidence interval (CI), $10,717-$25,400] compared with co-testing with hrHPV pooled primary and genotyped reflex testing, and $23,487 (95% CI, $15,745-$46,175) compared with co-testing with hrHPV genotyping with no reflex test. Screening and medical costs and life-years increased, while ICC costs and risk of ICC death decreased. Incorporating DS reflex into co-testing cervical cancer screening algorithms is projected to be cost-effective.</p><p><strong>Prevention relevance: </strong>The p16/Ki-67 dual-stained cytology (DS) test was recently approved in the United States as a reflex test for cervical cancer screening following positive high-risk human papillomavirus (hrHPV) test results. Adding DS reflex to hrHPV and cervical cytology co-testing strategies in the United States is expected to be cost-effective per life-year or quality-adjusted life-year gained.</p>","PeriodicalId":72514,"journal":{"name":"Cancer prevention research (Philadelphia, Pa.)","volume":"16 7","pages":"393-404"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/24/393.PMC10320467.pdf","citationCount":"0","resultStr":"{\"title\":\"Cost-effectiveness of p16/Ki-67 Dual-Stained Cytology Reflex Following Co-testing with hrHPV Genotyping for Cervical Cancer Screening.\",\"authors\":\"Diane M Harper, Rye J Anderson, Ed Baker, Tiffany M Yu\",\"doi\":\"10.1158/1940-6207.CAPR-22-0455\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The first biomarker-based cervical cancer screening test, p16/Ki-67 dual-stained cytology (DS), has been clinically validated and approved in the United States for triage of women being screened for cervical cancer who test positive for high-risk human papillomavirus (hrHPV). The primary aim of this work is to evaluate the cost-effectiveness of DS triage after co-testing findings of positive non-16/18 HPV types and atypical squamous cells of undetermined significance or low-grade squamous intraepithelial lesions cytology. A payer-perspective Markov microsimulation model was developed to assess the impact of DS reflex testing. Each comparison simulated 12,250 screening-eligible women through health states defined by hrHPV status and genotype, cervical intraepithelial neoplasia grades 1-3, invasive cervical cancer (ICC) by stage, and cancer-related or non-cancer death. Screening test performance data were from the IMPACT clinical validation trial. Transition probabilities were from population and natural history studies. Costs of baseline medical care, screening visits, tests, procedures, and ICC were included. DS reflex after co-testing was cost-effective with incremental cost-effectiveness ratios per quality-adjusted life-year gained of $15,231 [95% confidence interval (CI), $10,717-$25,400] compared with co-testing with hrHPV pooled primary and genotyped reflex testing, and $23,487 (95% CI, $15,745-$46,175) compared with co-testing with hrHPV genotyping with no reflex test. Screening and medical costs and life-years increased, while ICC costs and risk of ICC death decreased. Incorporating DS reflex into co-testing cervical cancer screening algorithms is projected to be cost-effective.</p><p><strong>Prevention relevance: </strong>The p16/Ki-67 dual-stained cytology (DS) test was recently approved in the United States as a reflex test for cervical cancer screening following positive high-risk human papillomavirus (hrHPV) test results. Adding DS reflex to hrHPV and cervical cytology co-testing strategies in the United States is expected to be cost-effective per life-year or quality-adjusted life-year gained.</p>\",\"PeriodicalId\":72514,\"journal\":{\"name\":\"Cancer prevention research (Philadelphia, Pa.)\",\"volume\":\"16 7\",\"pages\":\"393-404\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-07-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/24/393.PMC10320467.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer prevention research (Philadelphia, Pa.)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1158/1940-6207.CAPR-22-0455\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer prevention research (Philadelphia, Pa.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1158/1940-6207.CAPR-22-0455","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Cost-effectiveness of p16/Ki-67 Dual-Stained Cytology Reflex Following Co-testing with hrHPV Genotyping for Cervical Cancer Screening.
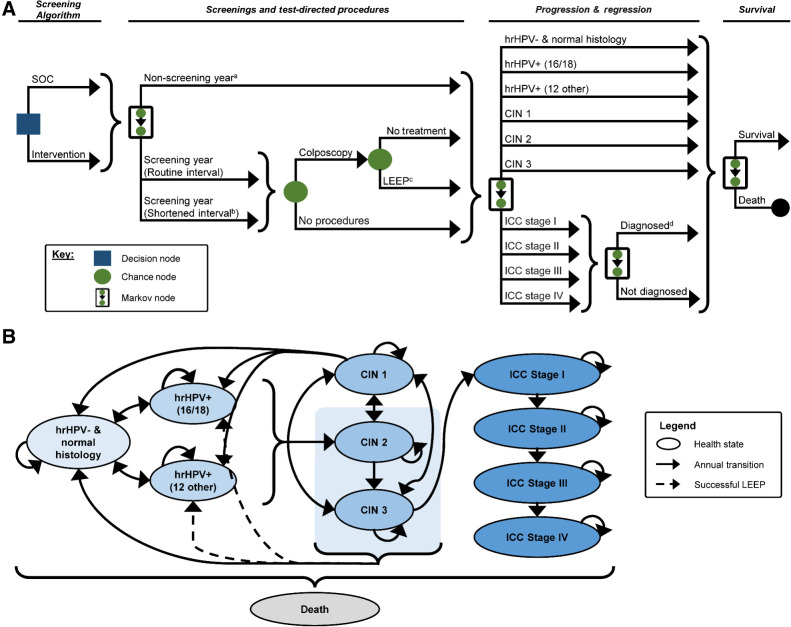
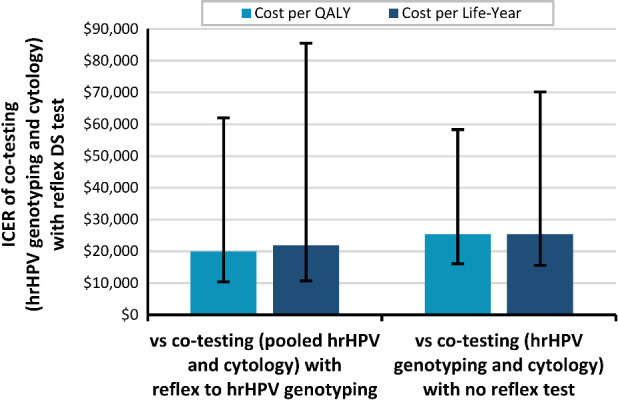
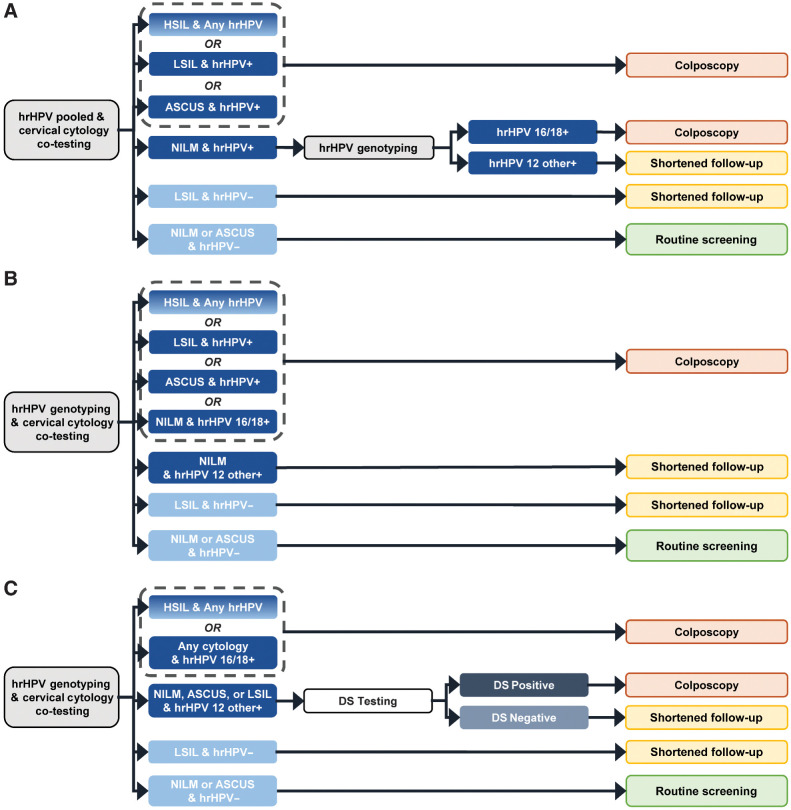
The first biomarker-based cervical cancer screening test, p16/Ki-67 dual-stained cytology (DS), has been clinically validated and approved in the United States for triage of women being screened for cervical cancer who test positive for high-risk human papillomavirus (hrHPV). The primary aim of this work is to evaluate the cost-effectiveness of DS triage after co-testing findings of positive non-16/18 HPV types and atypical squamous cells of undetermined significance or low-grade squamous intraepithelial lesions cytology. A payer-perspective Markov microsimulation model was developed to assess the impact of DS reflex testing. Each comparison simulated 12,250 screening-eligible women through health states defined by hrHPV status and genotype, cervical intraepithelial neoplasia grades 1-3, invasive cervical cancer (ICC) by stage, and cancer-related or non-cancer death. Screening test performance data were from the IMPACT clinical validation trial. Transition probabilities were from population and natural history studies. Costs of baseline medical care, screening visits, tests, procedures, and ICC were included. DS reflex after co-testing was cost-effective with incremental cost-effectiveness ratios per quality-adjusted life-year gained of $15,231 [95% confidence interval (CI), $10,717-$25,400] compared with co-testing with hrHPV pooled primary and genotyped reflex testing, and $23,487 (95% CI, $15,745-$46,175) compared with co-testing with hrHPV genotyping with no reflex test. Screening and medical costs and life-years increased, while ICC costs and risk of ICC death decreased. Incorporating DS reflex into co-testing cervical cancer screening algorithms is projected to be cost-effective.
Prevention relevance: The p16/Ki-67 dual-stained cytology (DS) test was recently approved in the United States as a reflex test for cervical cancer screening following positive high-risk human papillomavirus (hrHPV) test results. Adding DS reflex to hrHPV and cervical cytology co-testing strategies in the United States is expected to be cost-effective per life-year or quality-adjusted life-year gained.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


