{"title":"心源性休克的器官功能障碍、损伤和衰竭。","authors":"Akihiro Shirakabe, Masato Matsushita, Yusaku Shibata, Shota Shighihara, Suguru Nishigoori, Tomofumi Sawatani, Kazutaka Kiuchi, Kuniya Asai","doi":"10.1186/s40560-023-00676-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiogenic shock (CS) is caused by primary cardiac dysfunction and induced by various and heterogeneous diseases (e.g., acute impairment of cardiac performance, or acute or chronic impairment of cardiac performance).</p><p><strong>Main body: </strong>Although a low cardiac index is a common finding in patients with CS, the ventricular preload, pulmonary capillary wedge pressure, central venous pressure, and systemic vascular resistance might vary between patients. Organ dysfunction has traditionally been attributed to the hypoperfusion of the organ due to either progressive impairment of the cardiac output or intravascular volume depletion secondary to CS. However, research attention has recently shifted from this cardiac output (\"forward failure\") to venous congestion (\"backward failure\") as the most important hemodynamic determinant. Both hypoperfusion and/or venous congestion by CS could lead to injury, impairment, and failure of target organs (i.e., heart, lungs, kidney, liver, intestines, brain); these effects are associated with an increased mortality rate. Treatment strategies for the prevention, reduction, and reversal of organ injury are warranted to improve morbidity in these patients. The present review summarizes recent data regarding organ dysfunction, injury, and failure.</p><p><strong>Conclusions: </strong>Early identification and treatment of organ dysfunction, along with hemodynamic stabilization, are key components of the management of patients with CS.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"11 1","pages":"26"},"PeriodicalIF":4.7000,"publicationDate":"2023-06-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10308671/pdf/","citationCount":"0","resultStr":"{\"title\":\"Organ dysfunction, injury, and failure in cardiogenic shock.\",\"authors\":\"Akihiro Shirakabe, Masato Matsushita, Yusaku Shibata, Shota Shighihara, Suguru Nishigoori, Tomofumi Sawatani, Kazutaka Kiuchi, Kuniya Asai\",\"doi\":\"10.1186/s40560-023-00676-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiogenic shock (CS) is caused by primary cardiac dysfunction and induced by various and heterogeneous diseases (e.g., acute impairment of cardiac performance, or acute or chronic impairment of cardiac performance).</p><p><strong>Main body: </strong>Although a low cardiac index is a common finding in patients with CS, the ventricular preload, pulmonary capillary wedge pressure, central venous pressure, and systemic vascular resistance might vary between patients. Organ dysfunction has traditionally been attributed to the hypoperfusion of the organ due to either progressive impairment of the cardiac output or intravascular volume depletion secondary to CS. However, research attention has recently shifted from this cardiac output (\\\"forward failure\\\") to venous congestion (\\\"backward failure\\\") as the most important hemodynamic determinant. Both hypoperfusion and/or venous congestion by CS could lead to injury, impairment, and failure of target organs (i.e., heart, lungs, kidney, liver, intestines, brain); these effects are associated with an increased mortality rate. Treatment strategies for the prevention, reduction, and reversal of organ injury are warranted to improve morbidity in these patients. The present review summarizes recent data regarding organ dysfunction, injury, and failure.</p><p><strong>Conclusions: </strong>Early identification and treatment of organ dysfunction, along with hemodynamic stabilization, are key components of the management of patients with CS.</p>\",\"PeriodicalId\":16123,\"journal\":{\"name\":\"Journal of Intensive Care\",\"volume\":\"11 1\",\"pages\":\"26\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2023-06-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10308671/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40560-023-00676-1\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00676-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Organ dysfunction, injury, and failure in cardiogenic shock.
Background: Cardiogenic shock (CS) is caused by primary cardiac dysfunction and induced by various and heterogeneous diseases (e.g., acute impairment of cardiac performance, or acute or chronic impairment of cardiac performance).
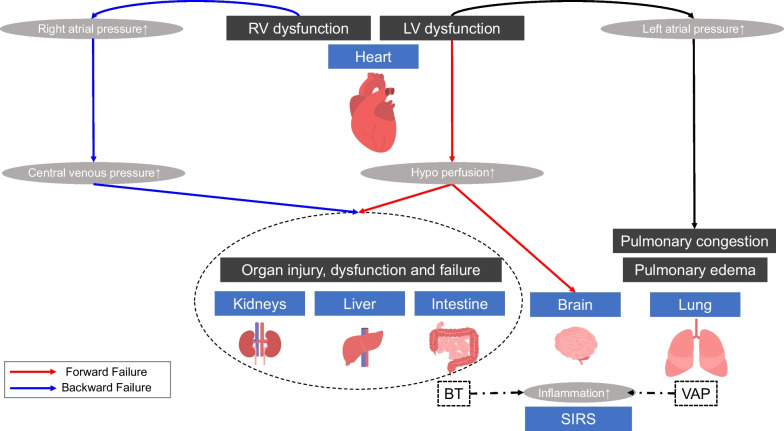
Main body: Although a low cardiac index is a common finding in patients with CS, the ventricular preload, pulmonary capillary wedge pressure, central venous pressure, and systemic vascular resistance might vary between patients. Organ dysfunction has traditionally been attributed to the hypoperfusion of the organ due to either progressive impairment of the cardiac output or intravascular volume depletion secondary to CS. However, research attention has recently shifted from this cardiac output ("forward failure") to venous congestion ("backward failure") as the most important hemodynamic determinant. Both hypoperfusion and/or venous congestion by CS could lead to injury, impairment, and failure of target organs (i.e., heart, lungs, kidney, liver, intestines, brain); these effects are associated with an increased mortality rate. Treatment strategies for the prevention, reduction, and reversal of organ injury are warranted to improve morbidity in these patients. The present review summarizes recent data regarding organ dysfunction, injury, and failure.
Conclusions: Early identification and treatment of organ dysfunction, along with hemodynamic stabilization, are key components of the management of patients with CS.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


